Senate Bill SB277, California’s draconian forced vaccination policy for school children in the public school system, will never see the light of day, if teachers and school administrators go on strike to oppose it. We, the people, (not our Government legislators), ‘have the real power.
If it comes to it, California should consider forming a sector of public schools across the State exclusively tailored for vaccine-free children. There are, conservatively, tens of thousands of eligible children ready to fill these seats.
This could be a turning point for our communities. I guarantee you, the positive ripple effects will quickly resonate throughout the Untied States, and elsewhere. Such is how we start bushfires of freedom in the hearts of our communities around the world.
The conflict looming in California, over the draconian, unlawful Bill, SB277, currently being instated, will have such serious consequences for families, we may be headed toward an open revolt, perhaps something akin to civil war.
Three crucial aspects to consider in respect to local communities affected:
1) Every parent or guardian is bound to protect their child’s inalienable right to self-determination of the body, what goes in it, and if so, administered by whom. The Government has no authority, whatsoever, to regulate, monitor or deny these primary parental rights.
2) It is unconstitutional to deny any child, born in the USA, their inherent right to free & open access to public education. This law therefore infringes on two crucial areas of basic freedom.
3) There will be hundreds of thousands of (unvaccinated) children displaced by this Bill. Their parents will be forced to homeschool their child/children; despite the fact that many of these families are two-income-type households.
California’s new forced vaccination Bill SB277, for children, represents the most draconian, fascist, unlawful health-directive ever to be forced upon the population in the history of the United States.
The whole premise behind personal exemptions was always a ruse.
The freedom to choose what goes into your, body, or into your child’s bloodstream, is non-negotiable. The Government has inverted and overturned this basic principle, and has, thus, bound freedom itself, to a contract.
Exemptions from Government imposed health mandates were ultimately designed to fail, by entrapping those members of the community who sign onto them, binding them to an arbitrary (constantly changing) list of choices (demands) that supercede said basic freedoms, and thereupon deny an individual their inalienable, God/life given rights to self-determination of the body.
Regardless of which way the pendulum swings, California is headed towards an imminent, all-out open revolt, nothing short of a groundswell civil war with the Government. Vaccine Resistance Movement

—————————————————————————————————————–—-

Such an accumulation of overlapping & contradictory scientific evidence begs the question – has the Medical community misdiagnosed Ebola?
Are we actually dealing with a virus here, or a bacterial strain, or in fact, a composite form of virus/bacteria hybrid?
Excerpts from VRM: Ebola Report
Why has the Ebola virus suddenly erupted in a region of Africa known as the “Meningitis Belt” (comprising all four countries affected – Guinea, Liberia, Nigeria & Sierra Leone)?
Because the WHO & CDC are deliberately trying to cover up their bloody tracks.
The recent Ebola outbreak in Africa coincides with a massive Meningitis Vaccine campaign targeting “150 million Africans”, many throughout Guinea & Nigeria.
The cost-effective vaccine, MenAfriVac®, (less than US$0.50 per dose) was “kept outside the cold chain for up to four days at up to 40°C”.
Neighboring Liberia & Sierra Leone, both primary epicenters, were recently subject to the “largest ever Yellow Fever Immunization Program” conducted in that region – an estimated 12 million locals impacted (infected) by the compound shot.
Vaccine Resistance Movement is investigating the link between these extremely toxic experimental vaccines and the sudden surge in cases of Ebola.

Symptoms of ‘Acute fulminating Meningococcal Septicemia’, a virulent form of bacterial meningitis (marked by extreme vomiting, hemorrhaging – excessive bleeding around the eyes & mouth, severe blackish bruising on the arms & legs), leading to Septic shock and potentially even death, closely resemble those seen in Ebola victims.
This supposed outbreak of Ebola bares all the hallmarks of a rarified, virulent strain of bacterial Meningitis, ‘Acute fulminating Meningococcal Septicemia’, also known as ‘Waterhouse-Friderichsen Syndrome’.
Is this yet another case of a dangerous, untested vaccine triggering a tsunami of viral & bacterial mutations – in impoverished regions?
Meningococcal Septicemia (Septic shock): ‘The hallmarks of severe sepsis and septic shock are changes that occur at the microvascular and cellular level with diffuse activation of inflammatory and coagulation cascades, vasodilation and vascular maldistribution, capillary endothelial leakage, and dysfunctional utilization of oxygen and nutrients at the cellular level. The challenge for clinicians is to recognize that this process is under way when it may not be clearly manifested in the vital signs or clinical examination.‘ Andre Kalil, MD, MPH Professor of Medicine, Department of Medicine, Section of Infectious Diseases; Director, Transplant ID Program, University of Nebraska Medical Center
Note: ‘DIC (Disseminated intravascular coagulation), is most commonly observed in severe sepsis and septic shock. Indeed, the development and severity of DIC correlate with mortality in severe sepsis. Although bacteremia, including both gram-positive and gram-negative organisms, is most commonly associated with DIC, other organisms (eg, viruses, fungi, and parasites) may also cause DIC.
DIC exists in both acute and chronic forms. Acute DIC develops when sudden exposure of blood to procoagulants (eg, tissue factor [TF], or tissue thromboplastin) generates intravascular coagulation. Compensatory hemostatic mechanisms are quickly overwhelmed, and, as a consequence, a severe consumptive coagulopathy leading to hemorrhage develops. Abnormalities of blood coagulation parameters are readily identified, and organ failure frequently results.‘ Marcel M Levi, MD Dean, Academic Medical Center, University of Amsterdam, The Netherlands
‘There is no evidence that MenAfriVac can cause meningococcal meningitis. Clinical alertness to the possibility of co-incidental meningitis should be maintained.‘ MenAfriVac® (Package insert)


The epidemiology of Yellow Fever also bares striking resemblance to Ebola, given the distinct characteristics & potential virulence common to each virus:
1. an incubation period lasting upwards of 1 week (‘Physical symptoms usually appear 3–6 days after’)
2. an array of flu-like symptoms during the initial stages, including (‘fever, muscle pain, particularly backache, headache, shivering, loss of appetite, and nausea or vomiting’)
3. leading to varying degrees of internal “blackish” bruising & widespread hemorrhaging (‘gastrointestinal bleeding, haematuria, skin petechiae, ecchymoses,’)
4. followed by rapid systemic deterioration, marked by Kidney failure, often leading to death (‘About 20%–50% of patients with hepato-renal failure die, usually 7–10 days after the onset of disease’)
About 20%–50% of patients with hepato-renal failure die, usually 7–10 days after the onset of disease. Patients surviving YF may experience prolonged weakness and fatigue, but healing of the liver and kidney injuries is usually complete.‘ Vaccines and vaccination against yellow fever/WHO Position Paper – June 2011

‘Yellow fever vaccine-associated viscerotropic disease (YEL-AVD) is clinically indistinguishable from wild-type yellow fever illness. Most YEL-AVD reports describe patients with fever and multiple organ system failure, and often death (17 deaths/29 cases worldwide).‘ The American Journal of Tropical Medicine and Hygiene

Even the CDC Director admits they are baffled by the unprecedented concentration of cases outside the typical range,
‘For more than four decades, Ebola virus had only been diagnosed in Central or Eastern Africa. Then late this past March, the first cases of Ebola began appearing in a surprising part of the continent. The outbreak in Guinea was the first sign that the virus had made the jump across the continent. Ebola then spread quickly to Sierra Leone and Liberia, and then to Nigeria.‘ Tom Frieden, MD, MPH, Director, US Centers for Disease Control and Prevention, Atlanta, Georgia
Irrespective of whether we are confronting a vaccine-derived hybrid (mutagenic) strain of bacterial Meningitis here, a vaccine-derived hybrid strain of Yellow Fever, or, in fact, a laboratory-derived hybrid strain of the Ebola Virus (essentially a composite of the laboratory produced Aids Virus) the so-called vanguard of Health “Authority”, chiefly the CDC & WHO, are purposefully focusing on a Vaccine & Drug response to this current health crisis, while ignoring the fact that the Ebola Virus can only thrive in a body starved of Selenium – thereby depriving our communities of critical information in a time of national emergency.
 The Ebola Virus can ONLY thrive in a body starved of Selenium. In fact ALL Ebola Virus victims, those who typically succumb to Hemorrhagic fever, viral replication (infected blood) and excessive hemorrhaging of the blood leading to death, concurrently suffer from acute malnutrition, marked by extreme Selenium deficiency in the body.
The Ebola Virus can ONLY thrive in a body starved of Selenium. In fact ALL Ebola Virus victims, those who typically succumb to Hemorrhagic fever, viral replication (infected blood) and excessive hemorrhaging of the blood leading to death, concurrently suffer from acute malnutrition, marked by extreme Selenium deficiency in the body.
Selenium is an essential anti-oxidant, the primary stop-gap which enables the human body to adapt to (overcome) any viral infections circulating in the environment, and prevents the typical Ebola-type symptoms (chiefly excessive hemorrhaging) from taking hold and ultimately killing the host (vaccinee).
Natural sources rich in Selenium include Brazil nuts, Sunflower seeds & Food Grade Diatomaceous Earth (“fossilized shell flour”).

If viruses like HIV-1 (Aids), coxsackievirus B3 (linked to Meningitis) and Ebola do encode selenoproteins, why does all the evidence suggest that dietary Se (Selenium) inhibits viral replication, whereas Se (Selenium) deficiency triggers replication?‘ Journal of Orthomolecular Medicine, 1995
Lipid peroxidation is associated with cellular damage resulting from oxidative stress (or Ischemia), which inhibits the capacity of cellular antioxidants, vital to natural immunity, by the unleashing of free radicals. – Scientific verification of demyelination linked to mitochondrial breakdown, caused by the intervention of (vaccine-derived) aluminum on early childhood development in the brain.

History is repeating itself…again.
Once again, just like in 2009, the WHO are purposefully inflating the numbers of victims here, to ensure the maximum fear factor is felt throughout our communities. Until those clinics & hospitals impacted by this crisis release the actual (post mortem) laboratory results, any statistics being foisted on us represent nothing more than speculation at best.
During the 2009 (CDC bio-laboratory produced) Pandemic. the WHO routinely exaggerated the overall death toll (attributable to H1N1); by including any/all cases associated with Flu-like symptoms – regardless of the fact that the VAST majority of victims inevitably died as a result of compromised immunity and/or pre-existing medical conditions. H1N1 was merely a blip on the radar, by all accounts a comparably mild seasonal flu.
It’s vitally important to analyze the current Ebola scare objectively. Throughout the recent manufactured “Swine Flu” Pandemic of 2009, communities around the world were manipulated constantly by Mainstream Media outlets (in lock-step with the WHO & spineless Government health departments), via an ongoing barrage of misinformation, negative hype & fear-mongering propaganda.
By the time all the dust settled it was unanimously determined by most experts in the scientific arena, “H1N1 has ultimately turned out to be, from a pandemic perspective, a dud.”
Fast-forward to 2014 … “As the (Ebola) epidemic gets more and more formidable and in some cases out of control it is quite conceivable, if not likely, that we may need to deploy the vaccine to the entire country to be able to shut the epidemic down. That is clearly a possibility.” U.S. National Institute for Allergy and Infectious Diseases (October 06, 2014)
Don’t allow yourself to be drawn into the propaganda. Within a year, this will, once again, be proven to have originated in a CDC Level 4 laboratory.
* Excerpts from VRM: Ebola Report
Lest we forget?

—————————————————————————————————————–—-
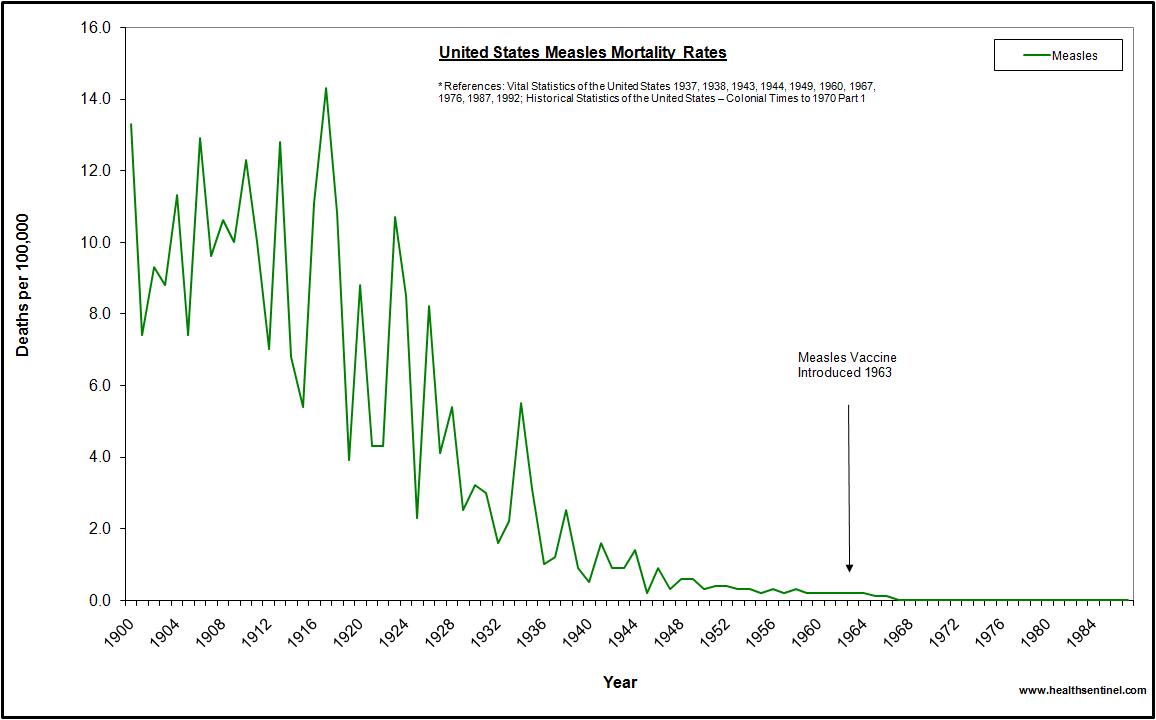
 Why are clusters of measles outbreaks on the rise? It has nothing to do with the increasing trend toward lower rates of vaccine uptake throughout our communities; the inference that avoiding getting your child “immunized” with the MMR series increases their risk of susceptibility to measles and transference of measles to other children in their proximity.
Why are clusters of measles outbreaks on the rise? It has nothing to do with the increasing trend toward lower rates of vaccine uptake throughout our communities; the inference that avoiding getting your child “immunized” with the MMR series increases their risk of susceptibility to measles and transference of measles to other children in their proximity.
As Dr Tetyana Obukhanych Ph.D, one of the world’s leading Immunologists (guest speaker at our recent VRM Vaccine Summit) points out, vaccines have stripped mothers, and by extension, their baby, of the capacity for life-long immuno-protection, given the absence of NATURAL childhood exposure to measles in the environment.
Parents who received the first wave of measles shots in 1963 (and all those since) were subsequently stripped of their capacity to transfer natural immuno-protection to their baby, via the Placenta & Colostrum, due to the cross-contamination factor (hybrid measles virus now embedded in the mother/father’s germ line DNA – manifesting in a more virulent strain of measles, known as ‘Atypical Measles’ or AMS) generated by the shot, passed on to the new generation.
The current generation have literally become unwitting hosts to a form of viral & bacterial roulette, an ideal breeding ground for the proliferation/weaponizing of viral & bacterial infections.

“I am very concerned that “immunologic memory” of adjuvant-containing vaccines is actually the basis of sensitization rather than the basis of immunity. Furthermore, I am very concerned that “successful” prevention of childhood diseases by means of short-term protective effects of live attenuated viral vaccines during childhood has led to the loss of maternal ability to transfer immuno-protection to their young, thereby leaving infants vulnerable to those diseases, should the exposure occur.
I am also very concerned that vaccination campaigns work by disrupting disease transmission, which reduces the chances of exposure, rather than by establishing a population’s immunity. By doing so, vaccination campaigns wipe out population’s immunity to childhood diseases rather than help to maintain it. If in prior decades there was naturally established herd immunity to childhood diseases among the adult population, then I am afraid that vaccination campaigns have ensured that it is long gone.
All of this is a direct outcome of the “desired” vaccination effects, the impact of which hasn’t been carefully thought through in advance of introducing mass vaccination. We thought that vaccines work just like natural immunity. Well, apparently they don’t and we are now reaping the consequences of that.
We would expect that vaccinated individuals would not be involved (or very minimally involved) in any outbreak of an infectious disease for which they have been vaccinated. Yet, when outbreaks are analyzed, it becomes apparent that most often this is not the case. Vaccinated individuals are indeed very frequently involved and constitute a high proportion of disease cases. I think this is happening because vaccination does not engage the genuine mechanism of immunity. Vaccination typically engages the immune response—that is, everything that immunologists would theoretically “want” to see being engaged in the immune system. But apparently this is not enough to confer robust protection that matches natural immunity. Our knowledge of the immune system is far from being complete.” Dr Tetyana Obukhanych Ph.D
The apparent paradox is that as measles immunization rates rise to high levels in a population, measles becomes a disease of immunized persons. Because of the failure rate of the vaccine and the unique transmissibility of the measles virus, the currently available measles vaccine, used in a single-dose strategy, is unlikely to completely eliminate measles. The long-term success of a two-dose strategy to eliminate measles remains to be determined.‘ Poland GA, Jacobson RM., Department of Internal Medicine, Mayo Vaccine Research Group, Mayo Clinic and Foundation, Rochester, MN./1994
In the meantime, outbreaks of measles in vaccinated children have continued and intensified to this day. Contemporary observations of the ineffectiveness of vaccination indicate to me that the incidence of measles has increased and has not continued decreasing as it did for some 100 years before any type of measles vaccination was introduced.‘ Dr Viera Scheibner (PhD), International Medical Counsel on Vaccination

Measles, Mumps, Rubella Vaccine (series) – 1st round given at 12-15 months old: ‘The evidence convincingly supports a causal relationship between MMR vaccine and measles inclusion body enchephalitis (inflammation of the Brain & Meninges/Meningoencephalitis manifesting as ‘diffuse and/or focal neuropsychological dysfunction‘ – reaction to synergistic heavy metal-excipient accumulation of ’sludge’ toxicity) in individuals with demonstrated immune deficiencies.’ P.110 Institute of Medicine Report on Adverse Effects of Vaccines/2011‘
A mutagenic Measles virus strain commonly infects the bowels/intestines of children with Autism. Merck’s official package insert for the Measles, Mumps, Rubella vaccine explains why: ‘M-M-R II has not been evaluated for carcinogenic or mutagenic potential, or potential to impair fertility.‘
‘Measles vaccine can cause problems (e.g. fatal giant cell pneumonia) in those with severely compromised cell-mediated immunity.‘…”I have also found that regressive behavioral disorder (RBD) in children is associated with measles, mumps and rubella (MMR) vaccination. These children all have gastrointestinal symptoms including abdominal pain, diarrhea, and in some cases food intolerance. It is significant that this syndrome only appeared with the introduction of the polyvalent MMR vaccine in 1988 rather than with the monovalent measles vaccine introduced in 1968. This indicates that MMR is responsible for this condition rather than just the measles virus and that accordingly a transfer factor specific for the components other than the measles virus in MMR may be required.” Dr. Andrew Wakefield
‘One study, in which autopsied elderly were examined for the presence of the measles virus, found that 20% of the brains had live measles viruses and 45% of other organs were infected. These viruses were highly mutated, meaning that they could be just as potent as other measles viruses, but could be even more virulent. Worse, is that in most cases they cause a smoldering destruction of tissues without the obvious symptoms of infection, which has been shown in a number of studies.’ Dr. Russell L. Blaylock
Note: Dr. Andrew Wakefield’s 1998 Study demonstrated “anti-myelin antibodies and digestive tract pathologies in children with autism after being given the Urabi strain triple live virus MMR vaccine. All 12 children in the Study had intestinal abnormalities (known as Inflammatory Bowel Disease), with chronic inflammation in the colon in 11 of the children. Noted behavioral disorders included autism in 9, disintegrative psychosis in 1, and possible post-viral or vaccinal encephalitis (acute brain inflammation) in 2.
Since that release there have been countless other studies verifying exactly the same pattern – including the presence of measles lingering in the bowels of young children who have gotten of the Measles-Mumps-Rubella shot (MMR).
The Urabi strain MMR vaccine purchased by GlaxoSmitheKline for distribution in the UK, a triple live virus version, was directly responsible for an sudden spike in childhood Meningitis in the UK. It had been banned from use in Canada & was warned against further use in Britain by Canadian specialists. This was all suppressed by GSK & The British Gov’t. They are solely to blame for this crisis.

Government data admits to a probable causal link between vaccines & the presence of Measles in the bowels of young children (related to Inflammatory Bowel Disease); while promoting a deliberate cover-up of these inherent risks to the general public,
‘That Crohn’s disease and other chronic inflammatory illnesses of the intestine might be caused by a virus such as measles is an interesting hypothesis. Until the present time, microbiologic and epidemiologic arguments either for or against this hypothesis have not been very convincing. It is not very likely that other epidemiologic studies will provide conclusive evidence. In fact, it would be difficult to find a population that includes both individuals who have been exposed to the virus or to the vaccine and individuals who have not been exposed. However, new microbiologic studies might prove conclusive.
First, it would be necessary to demonstrate that the measles virus is indeed present in the lesions, that it is active, and that it contributes to inflammatory responses. Also, it would be necessary to prove that the pathogenic reaction can be induced by the wild virus and by the attenuated viruses present in vaccines. Strains and attenuation procedures vary from one manufacturer to another, and it is far from certain that all strains have the same ability to persist in tissues and to subsequently produce chronic inflammations. As was stated above, measles vaccine does not seem to be associated with SSPE, although the wild virus may be isolated (with difficulty) in patients with SSPE. The measles virus was isolated neither in patients with Crohn’s disease or other chronic inflammatory diseases (Paget’s disease, active chronic hepatitis, multiple sclerosis) in which a role for it has been claimed on morphologic, histologic or serologic grounds.
Current scientific data do not permit a causal link to be drawn between the measles virus and chronic inflammatory bowel diseases. While awaiting production and publication of other research, it would not be appropriate to alarm recipients of the vaccine by notifying them of this hypothetical risk, thus jeopardizing an immunization program of proven benefit.’ Public Health Agency of Canada
Scandalous cover-up: “…it would not be appropriate to alarm recipients of the vaccine by notifying them of this hypothetical risk, thus jeopardizing an immunization program of proven (cost) benefit.”
‘Despite the advantages of live, attenuated vaccines, there are some downsides. It is the nature of living things to change, or mutate, and the organisms used in live, attenuated vaccines are no different. The remote possibility exists that an attenuated microbe in the vaccine could revert to a virulent form and cause disease.‘ US National Institute of Allergy and Infectious Diseases
“One vaccine decreases cell-mediated immunity by 50%, two vaccines by 70%…all triple vaccines (MMR, DTaP) markedly impair cell-mediated immunity, which predisposes to recurrent viral infections, especially otitis media, as well as yeast and fungi infections.” World-renowned Immunologist Dr. H.H. Fudenberg
Excerpts from VRM: MEASLES REPORT
See VRM: The Rise of Mutagenic Viruses
See VRM: The Autism Report http://vaccineresistancemovement.org/?p=10185
Vaccine Resistance Movement
—————————————————————————————————————–—-

Every Vaccine in circulation is required to undergo Clinical Trials before being granted sale onto the market. The Vaccine Industry uses a statistical measure called “relative risk” (rather than “absolute risk”) to deliberately bury/obfuscate any direct causal link between the vaccine itself and subsequent neurological & neurodevelopmental damage incurred.
This enables them to minimize or eliminate altogether, the extent of negative trial data potentially hindering the glowing track-record of the product. Therefore, any/all cases of Sudden Infant Death, Encephalitis, Anaphylaxis, Seizures, etc. etc. etc….detected in the hours/days post inoculation, are never recorded in the final analysis (equation), cancelled out by the total number of percentages. It’s nothing but a shell game.
‘An important feature of relative risk is that it tells you nothing about the actual risk. This can be very important for evaluating how significant a relative increase might be.‘ George Mason University
—————————————————————————————————————–—-
THE DARK HISTORY OF THE HEPATITIS B VACCINE – 3 doses given, 1st round administered at 12 hours old (after birth):
 Research scientists have now identified a direct causal link between subcutaneous &/or intramuscular injection of the Hepatitis B Vaccine and resulting Mitochondrial dysfunction (hallmark symptom of Autism); including premature apoptosis or “programmed” type cell death. Hep B vaccine factors into eventuality of Early Onset Autism, since it represents the earliest premature breach of a baby’s delicate, under-developed “electrical grid system” (Myelin sheath, Meninges & Blood Brain Barrier).
Research scientists have now identified a direct causal link between subcutaneous &/or intramuscular injection of the Hepatitis B Vaccine and resulting Mitochondrial dysfunction (hallmark symptom of Autism); including premature apoptosis or “programmed” type cell death. Hep B vaccine factors into eventuality of Early Onset Autism, since it represents the earliest premature breach of a baby’s delicate, under-developed “electrical grid system” (Myelin sheath, Meninges & Blood Brain Barrier).
WILLOWBROOK STATE SCHOOL FOR MENTALLY CHALLENGED (Staten Island, NY )/196O’s – Mentally challenged students (inmates) were forcibly injected with cancerous Hepatitis B shots. Thousands infected, hundreds died.

How much better to have a patient with hepatitis accidentally or deliberately acquired under the guidance of a Krugman, than under the care of a rights-minded zealot.”‘ Excerpt from Carol Rutz’s Lecture at Indiana University, November 2003
‘Exposure of Hepa1-6 cells to a low dose of adjuvanted hepatitis B vaccine leads to loss of mitochondrial integrity, apoptosis induction, and cell death…‘In vivo apoptotic effect of hepatitis B vaccine was observed in mouse liver.‘…’Boys vaccinated as neonates had threefold greater odds for autism diagnosis compared to boys never vaccinated or vaccinated after the first month of life. Non-Hispanic white boys were 64% less likely to have autism diagnosis relative to nonwhite boys. Findings suggest that U.S. male neonates vaccinated with the hepatitis B vaccine prior to 1999 (from vaccination record) had a threefold higher risk for parental report of autism diagnosis compared to boys not vaccinated as neonates during that same time period.‘
Official Package Insert: ‘10 µg/mL Each 1 mL dose of sterile suspension contains hepatitis B surface antigen 10 µg adsorbed onto approximately 0.5 mg of amorphous aluminum hydroxyphosphate. Formaldehyde-treated. Thimerosal (mercury derivative) 1:20,000 (50 µg/mL) has been added only to the preservative-containing formulations. 3-dose vials of 3 mL‘…’A portion of the hepatitis B virus gene, coding for HBsAg, is cloned (synthetic genomics) into yeast, and the vaccine for hepatitis B is produced from cultures of this recombinant yeast strain.‘
Think about it. Vaccine Resistance Movement
—————————————————————————————————————–—-

The Flu Vaccine deception ranks as one of the great cover-ups & swindles of the last century perpetrated against the general population. Not only has the public been systematically lied to by their elected Gov’t for generations (in league with the World Health Organization & a Vaccine Industry Medical Mafia feeding trough), but the entire bedrock of our natural immunity has been put at risk through the collision of forces being pitted against us around the world.
The business of the Vaccine Industry represents a multi-billion dollar enterprise, and countries around the world (194 signatory nations under the banner of a World Health Organization treaty) are literally “bound” to this bottomless swindle – our communities the intended “target market” fodder. ‘The International Health Regulations (IHR) is an international legal agreement that is binding on 194 States Parties across the globe, including all of the Member States of WHO.‘
Once again this year, Government “Health Officials” & Mainstream Media outlets are in unison, using the same desperate tactics they employed during 2009, the marketing ploy of “artificial scarcity”, withholding vaccine supplies long enough to create the PERCEPTION of a shortage, while reinforcing the myth of herd immunity compliance locally; banner headlines of crowds “flocking” to emptied-out clinics, panic everywhere, all in a desperate attempt to frighten the public into getting the Flu shot.
Just remember, 65-70% of our community are REFUSING to get the Flu shot every year. Statistically, 70% of Canadians are REFUSING to get the Flu shot every year…only 30% of Canadians in compliance (based on Statistics Canada: Annual rates): 25-28% of males get the flu shot, while 30-33% of females get the flu shot.
The current US influenza vaccination rate (for all adults 18 years and older) ranges from ’28.0% to 36.2%.‘


1. Flu deaths are attributed primarily to bacterial pneumonia triggered by the flu symptoms. The flu itself cannot kill you
2. Most victims of the flu are those 65 years and older
3. In almost every instance a compromised immune system is a key factor in those victims who succumb to the flu
4. Most children who succumb to seasonal Flu, either via death or serious long-term illness (in particular those tracked since 2009), are subsequently found to have been 8 times more predisposed to a Methicillin-resistant Staphylococcus Aureus (MRSA) bacterial co-infection occurring in the lungs.
It is also significant that routine prescription anti-bacterials/virals (chiefly Vancomycin Hydrochloride Capsules & Oseltamivir/Tamiflu), widely distributed globally to ostensibly combat flu-like symptoms, have in fact been the tipping point which has worsened such conditions, hastening Kidney failure, Myocarditis (inflammation of the Heart Muscle) & numerous instances of sudden death.
Think about it. Vaccine Resistance Movement

A growing number of children with Autism are now potentially cross-infected with SV40 (diseased African Green Monkey kidney derived Polio virus) type hybrid strains of Poliomavirus (67% infection with Simian Virus); based on a recent Controlled Study which found poliomavirus infection in postmortem brains of sufferers of Autism – inevitably the result of inter-generational cross-contamination from Salk & Sabin Polio inoculations, sugar cube/oral drops versions & the subsequent Inactivated Polio Vaccine now on the schedule; fixed in the germline DNA of babies/children.
Note: ‘simian retrovirus (SRV) was present as genetically defective DNA.’
Please consider supporting the ongoing efforts of VRM in awakening our communities to Vaccine Industry malfeasance & the paradigm shift toward self-sufficiency & holistic health.
The Vaccine Resistance Movement is finally in a position to reach families throughout the community with this powerful message of self-sufficiency & key steps to take in the paradigm shift toward self-determination of the body…
This important gathering marked the first big push forward following our recent VRM Vaccine Summit. The VRM Silent No More Project brings together some of the same parents of vaccine-injured children in a more intimate setting. Vaccine Researcher Joel Lord also conducts an extensive presentation on the Autism epidemic, synergistic toxicity, demyelination & blood-brain barrier threshold in babies, with a detailed Powerpoint presentation. 2 disks and over 4 hours of ground-breaking footage.
Anyone in the community able to donate $25 or more to VRM will be honoured with a personal, signed copy of the upcoming ‘VRM: Silent No More Project’ DVD – while supplies last. Ongoing availability of this release to a wider community is contingent on us reaching a minimal goal of financing. So I am reaching out to you now.
For those able to donate $50 or more, I will send you a signed copy of the bound booklet version The VRM Autism Report or The Problem With Vaccines Part 4 – Primary Aspects of Vaccine Toxicity Affecting The Body, both of which have been expanded for this special edition (while supplies last); in addition to a signed copy of the VRM Silent No More Project DVD.
For donations of $100 or more I will send you a signed copy of the bound booklet version The VRM Autism Report plus The Problem With Vaccines Part 4 – Primary Aspects of Vaccine Toxicity Affecting The Body, both of which have been expanded for this special edition (while supplies last); in addition to a set of signed copies of the VRM Silent No More Project DVD.
Please see the orange tab Paypal link on the VRM website (click on ‘Donate Online’). Thank you all. Joel Lord, founder of The Vaccine Resistance Movement
—————————————————————————————————————–—-
A great inspiration of mine has just passed away. Dr. Andrew Moulden, an extraordinary font of knowledge who challenged the entire basis of vaccination using the science of the body, a true pioneer in the field of vaccine research, who broke through all the Industry lies & rhetoric by identifying the root cause in ALL cases of vaccination-induced neurological & neurodevelopmental trauma…Ischemia.
If it weren’t for Dr. Andrew Moulden’s extraordinary research, I would never have found my way to the heart of the matter as a vaccine researcher.
The viscosity of this toxic sludge resulting from vaccines which accumulates in the organs (ie. heart, liver, kidney, spleen), joints, meninges, intestines, along the neural pathways, veins & capillaries interlacing the entire body (resulting from “stagnant” blood), is comparable to the black paste-like build-up found over time in the lining of your drains – especially in terms of its impact on your vital health.
Within 72 hours of oxygen deprivation any cell can become cancerous. Cancer cells thrive in an oxygen-deprived environment. This will occur when bio-conductive aluminum (consisting of live virus, antibiotic, heavy metal, detergent coagulated sludge) clogs/singes the vast network of arterial veins & capillaries leading to the brain, inducing Ischemia.
Here’s one of those rare moments captured when a brilliant mind, unfettered by mainstream academic dogma, soars on the wings of truth.
http://www.youtube.com/watch?v=D5ApDkvCNQo
‘During times of universal deceit, telling the truth becomes a revolutionary act.’ George Orwell
Andrew, may you rest in peace.
Vaccine Resistance Movement
—————————————————————————————————————–—-

The only purpose for modern hospitals should be that of promoting the betterment of life (including that of life-saving triage surgery).
Instead, most current hospitals are designed primarily to further the massive profits of Institutionalized long-term “chronic” care & Western Allopathic ‘”symptom-based” Medicine.
When was the last time a major hospital explained to a family the benefits of using apple cider vinegar & baking soda, or handed out samples of curcumin, apple, apricot & pumpkin seeds, or Burdock Root, or nascent iodine…or invested in Hyperbaric Oxygen chambers instead of more CT Scanning machines & chemotherapy wards…
Use of CT Scans for Cancer Diagnosis/Treatment: ‘Computed tomography (CT) is a diagnostic procedure that uses special x-ray equipment to obtain cross-sectional pictures of the body. In cancer, CT is used to detect a tumor, provide information about the extent of the disease, help plan treatment, and determine whether the cancer is responding to treatment. A CT scan uses slightly more radiation than a chest x-ray, but the benefits generally outweigh the risks.’ National Cancer Institute
‘Hospitals Performed Needless Double CT Scans, Records Show: In 2008, about 75,000 patients received double scans, one using iodine contrast to check blood flow, and one that did not. “If you do both, you bill for both,” Dr. Pentecost said. A single CT scan of the chest is equal to about 350 standard chest X-rays, so two scans are twice that amount.’ New York Times
Note discrepancy: ‘A CT scan uses slightly more radiation than a chest x-ray (NCI) VS. ‘A single CT scan of the chest is equal to about 350 standard chest X-rays (NYT)
Hyperbaric Oxygen Therapy (HBOT) rapidly eradicates cancer cell growth & quickly restores cell vitality to effected areas in the body without the toxic side-effects associated with Conventional Western Allopathic methods (ie. Chemotherapy); however it is not being applied readily or effectively where it is needed most. ‘Some, but not very many, hospitals have a hyperbaric chamber. Smaller units may be available in outpatient center.‘ This despite the fact that it can be made cost effective for patients, with promising results currently demonstrated in Britain.
‘We just finished HBOT with our son…had improvements in fine and gross motor skills as well as RECEPTIVE language. We did an hour a day from May 2011 until this month.’ VRM member, parent of child coping with Autism
—————————————————————————————————————–—-


‘Canada needs a national vaccination registry so no child misses out on being immunized. A registry would help the government track how many people across the country have been vaccinated. There’s also a need for a co-ordinated national campaign to counter anti-vaccine voices.‘ Canadian Public Health Association
In the US, on average, only 35% of children are receiving the flu shot every year, 25-30% of adults, 63% of seniors over 65 – an indication of growing distrust in immunization policy as a means of strengthening immunity. ‘If the trend continues this season, overall coverage will still remain substantially below the Healthy People 2020 influenza vaccination targets.‘ CDC
Vaccine Resistance Movement
See VRM: 5 Reasons Not To Get The Flu Shot
See VRM: Pandemic Preparedness & The Dark Agenda Ahead
—————————————————————————————————————–—-
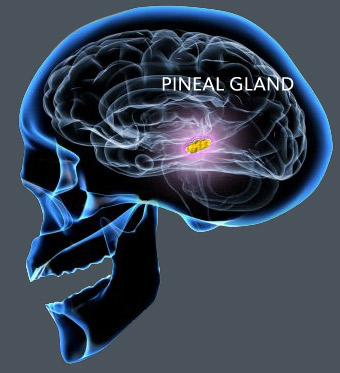 Melatonin & The Pineal Gland:
Melatonin & The Pineal Gland:
The Pineal Gland, considered the master gland, which oversees the entire process of metabolic function in the body, ‘five times superior to glutathione in scavenging free hydroxyl radicals‘ (referred to as the ‘third eye’ in ancient cultures), traditionally grew to the size of a quarter in the human body, before the introduction of sodium fluoride into the water supply & widespread use in toothpaste products – when natural immunity could thrive unhindered by such toxic detritus.
Today, the average size of the Pineal Gland in most consumers in the west has diminished to that of a withered dime.
‘The pineal gland is innervated by sympathetic axons and by axons coming directly from the brain. Besides sympathetic innervation, the pineal gland receives axons directly from the brain that enter through the stalk. The function of these fibers relative to the physiology of the pineal is unknown.‘ Vollrath L. Functional anatomy of the human pineal gland
We have recently discovered that it stimulates two major hormones called serotonin and melatonin.
 The Thyroid Gland is critical in the body. The extent of its ability to function normally determines your degree of overall heath. It is a bell weather indicator. A compromised immune system is much more vulnerable to infection & seasonal influenza. Vaccines target/undermine the Immune system by introducing live viruses & toxic heavy metals to an already overloaded network; systematically stripping the body of its capacity to harness vital trace minerals (chiefly Selenium, Zinc, Magnesium) & antioxidants (chiefly Vitamins A, B6/B12, C, D3, E + Glutathione).
The Thyroid Gland is critical in the body. The extent of its ability to function normally determines your degree of overall heath. It is a bell weather indicator. A compromised immune system is much more vulnerable to infection & seasonal influenza. Vaccines target/undermine the Immune system by introducing live viruses & toxic heavy metals to an already overloaded network; systematically stripping the body of its capacity to harness vital trace minerals (chiefly Selenium, Zinc, Magnesium) & antioxidants (chiefly Vitamins A, B6/B12, C, D3, E + Glutathione).
The synergy of immunological, neurological & physiological well being hangs in the balance. Thus the delicacy of our glands must be protected. Otherwise a domino effect of sickness & long term deterioration of health are inevitable.
‘It is known that melatonin scavenges oxygen and nitrogen-based reactants generated in mitochondria. This limits the loss of the intramitochondrial glutathione and lowers mitochondrial protein damage.‘ León J, Acuña-Castroviejo D, Escames G, Tan DX, Reiter RJ., Department of Cellular and Structural Biology, University of Texas Health Science Center, San Antonio, TX
Note: Any product that replicates a naturally occurring substance in the body, such as Melatonin supplement, should be used sparingly, as it can undermine the effectiveness of the Thyroid Grand, by unleashing an over-abundance of free-radicals, triggering hyper/hypothyroidism. Just be prudent, and monitor your health effects on a day-to-day basis, or that of your child, while on these products. Holistic health requires constant attention to the delicate balance of myriad inter-dependent systems at work; otherwise you’ll often cause a chain reaction elsewhere, by overloading or over-stimulating one component of the body.
Vaccine Resistance Movement
—————————————————————————————————————–—-

The cream of the crop in the Medical community are immediately sought after in Medical School by Vaccine Manufacturing giants long before they graduate, with the eventual promise of scientific research grants, lucrative payoffs & promotions for product endorsements at medical seminars, through the commissioning of fraudulent clinical trials, including the luxury of all expenses paid weekend getaways, and other incentives once they graduate to top positions in major hospitals & clinics (such as unlimited access to free samples & donated medical equipment).
In return, these obliging doctors must tow the line and push these Vaccines on our communities, without reservation. For some, whose values were compromised early enough, the original meaning of the Hippocratic Oath, “Thou Shalt Do No Harm” has long since lost to the lustre, the lure and the prestige afforded by the almighty dollar.
Regrettably, most Pediatricians are completely in dark on these crucial aspects of vaccine-derived synergistic heavy metal/excipient derived toxicity associated with early childhood immunization, the acute vulnerability of a baby’s brain & central nervous system properties (Myelin Sheath, Blood-brain barrier, Meninges). Almost all mainstream Pediatricians are loathe to promote the benefits of holistic health, as it contravenes the bottom line business practice of peddling prescription drugs & vaccines on the community at large. Self-reliance & optimal natural immunity is not in their best interest.
Their education is specifically limited & tailored to the scope of that which supports the advancing of the Industry food-chain of profits, under the banner of “herd immunity”. The human cost is typically overlooked and under-reported. This wide gulf in understanding can be explained.
According to Dr. Russell Blaylock, world renowned former brain surgeon, the average doctor receives the equivalent of a weekend seminar, in their first year only, on the specific topic of the neurological side-effects & disorders associated with vaccine uptake; approximately seven hours of careful, focused study into the complex strata of auto-immune breakdown type complexities. Without this fundamental bedrock of knowledge a critical component is missing from any doctor’s arsenal, considering the widespread impact neurological side-effects to vaccines have had on the community at large.
‘No medical man during his student days is taught to think. He is expected to assimilate the thoughts of others and to bow to authority. Throughout the whole of his medical career he must accept the current medical fashions of the day or suffer the loss of prestige and place. No public appointments, no coveted preferments are open to the medical man who declines to parrot the popular shibboleths of his profession. His qualifications may be beyond reproach, he may in himself possess qualities that command respect, but unless prepared to think and act within the narrow circle of accepted dogmas, he must be prepared for a more or less isolated path.’ Dr. Walter Hadwen, M.D., UK
Vaccine Resistance Movement
—————————————————————————————————————–—-
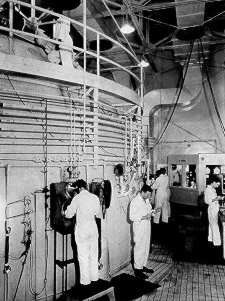
VRM Breaking News – Buried history finally uncovered. The founder of Merck & Co., manufacturer of the HPV Vaccine ‘Gardasil’, was also former chairman of the Biological Warfare Committee of the US Army Chemical War Service during WW2

George W. Merck, grandson of Heinrich Emanuel Merck (founder of the German-based drug-manufacturing firm ‘E. Merck AG’), took over the US branch of the pharmaceutical firm, known as ‘Merck & Co.’, in 1925. According to officially “withdrawn” documents (see Keesing’s Contemporary Archives, London, February 2-9, 1946), George W. Merck was appointed ‘Official chairman of the Biological Warfare Committee of the US Army Chemical Warfare Service’, during WW2. In 1942 he was authorized, by President Roosevelt, to study & manufacture biological weaponry for the US Military.
 ‘The idea of biological weaponry was controversial, since little was known about the predictability or effectiveness of biological weapons in wartime. President Roosevelt approved the plan in 1942, and the War Reserve Service, headed by George W. Merck, was established and attached to the Federal Security Agency, a New Deal agency of the Department of Agriculture. The War Reserve Service started out in mid 1942 with a budget of $200,000. Secret work began under Merck’s direction at 28 American universities, including Harvard, Stanford, and other top schools. This agency received consultative advice from national scientific committees and organizations, including the National Academy of Sciences and the National Research Council.
‘The idea of biological weaponry was controversial, since little was known about the predictability or effectiveness of biological weapons in wartime. President Roosevelt approved the plan in 1942, and the War Reserve Service, headed by George W. Merck, was established and attached to the Federal Security Agency, a New Deal agency of the Department of Agriculture. The War Reserve Service started out in mid 1942 with a budget of $200,000. Secret work began under Merck’s direction at 28 American universities, including Harvard, Stanford, and other top schools. This agency received consultative advice from national scientific committees and organizations, including the National Academy of Sciences and the National Research Council.
 The War Reserve Service also empowered the U.S. Army’s Chemical Warfare Service to greatly expand its efforts in regard to biological weapons. The army’s efforts were better funded than those of the War Reserve Service: in 1942 and 1943, the Chemical Warfare Service received millions of dollars to build research facilities. Several locations were selected for the army’s biological research, with the main headquarters at Camp Detrick, Frederick, Maryland, a small National Guard airfield (designated Fort Detrick in 1956).
The War Reserve Service also empowered the U.S. Army’s Chemical Warfare Service to greatly expand its efforts in regard to biological weapons. The army’s efforts were better funded than those of the War Reserve Service: in 1942 and 1943, the Chemical Warfare Service received millions of dollars to build research facilities. Several locations were selected for the army’s biological research, with the main headquarters at Camp Detrick, Frederick, Maryland, a small National Guard airfield (designated Fort Detrick in 1956).
The army also made plans to build a manufacturing plant near Terre Haute, Indiana, and built a 2,000-acre field test site on Horn Island in Pascagoula, Mississippi. It is ironic that much of the United States’s biological warfare effort during World War II was in response to a perceived threat from Germany, when in fact the Japanese were much more actively building their biological warfare capability.’ THE U.S. BIOLOGICAL WARFARE AND BIOLOGICAL DEFENSE PROGRAMS/DAVID R. FRANZ, D.V.M., PH.D.; CHERYL D. PARROTT; & ERNEST T. TAKAFUJI, M.D., M.P.H. http://ww.phsource.us/PH/CBRNE/MABCW/Ch19.pdf
See VRM: Gardasil/Cervarix – A Legacy Of Shame
See VRM: Gardasil/Cervarix Part 2 – Demyelination, Multiple Sclerosis & the Copaxone Connection
—————————————————————————————————————–—-
The modern healthcare system, like any powerful corporation, is designed to favor those who acquiesce with their rules & regulations; likewise to weed out & alienate those who do not fall into line with the rest of the “herd”. The entire cesspool of Western Allopathic Medicine, fueled by a medical mafia monopoly, dominates our lives through an endless barrage of mainstream media propaganda, a giant social engineering model, run by select commitees of overpaid Technocratic Elites – void of any decent moral code of ethics, adherence to the Hippocratic oath or underlying sense of altruism toward humanity. How do we avoid their calibrated landmines, and retain what little we can of self reliance and self-sustaining capacity for natural immunity in these tyrannical times? We must reluctantly go along with their manufactured guidelines, in order to stand clear from the rest of the herd.
It is important to understand that ANY/ALL exemptions pertaining to standard immunization vaccines (medical, religious or moral/personal belief type) are fundamentally illegal, because they tranpose an inherent human RIGHT into a PRIVILEGE, on the presumption that you acknowledge and thus sacrifice your natural born “freedom of choice” to an external authority. This is the basis of the looming collectivist (authoritarian) model being rolled out worldwide – the complete isolation of non-conformists and critical thinking individuals. Just remember, it is all color of law, technically a form of entrapment. Eventually they will tighten the noose, and cut everyone off from independent options altogether. In order to attain an education, in order to maintain a job, in order to enter a hospital or clinic, in order to go shopping, in order to travel, in order to live amongst others (including your family) within any community, ultimately in order to function on any practical level within society, you will be FORCED to get your shots.
Mandatory vaccinations are being phased in incrementally, by stealth, through this co-ordinated, systemic process of passive aquiescence. Once the “cashless grid” police state infrastructure is firmly in place, worldwide, EVERY citizen (excluding those Elites who manage the populace from on high), will be forced to submit to all standard immunization protocols by LAW (including Government/CDC issued “pandemic shots” inevitably designed to sterilize the host) on penalty of forfeiture/suspension of their vital carbon credit allotment. So it is now emcumbant upon you as an individual to decide the course of your future. Are you going to serve the corporation…and join the herd, or stand by your family? Think about it. VRM
Eli Lilly and Company: Thimerosal/Material Safety Data Sheet – ‘Thimerosal contains 49.6% w/w organically-bound mercury. Exposure Guidelines: Thimerosal – No known occupational exposure limits established. Early signs of mercury poisoning in adults are nervous system effects, including narrowing of the visual field and numbness in the extremities. Exposure to mercury in utero and in children may cause mild to severe mental retardation and mild to severe motor coordination impairment.’
‘A single thimerosal-containing vaccination produces acute ethylmercury blood levels of 10–30 nM (nanomolar concentration), and blood samples in 2-month-old infants, obtained 3–20 days after vaccination, contain 3.8–20.6 nM ethylmercury. Our studies therefore indicate the potential for thimerosal to cause adverse effects on MS (methionine synthase – determines the viability of cells) activity at concentrations well below the levels produced by individual thimerosal-containing vaccines.’ M Waly, H Olteanu, R Banerjee, S-W Choi, JB Mason, BS Parker, S Sukumar, S Shim, A Sharma, JM Benzecry, V-A Power-Charnitsky, RC Deth – See page 10
Aluminum, combined with other ingredients commonly added to vaccines, will trigger more rapid & profound cell toxicity. Mercury, another devastating neurotoxin & one of the few liquid elements, actually binds with hemoglobin, which is responsible for oxygen transport to the tissues. In addition it “inhibits the regulation of brain glutamate levels, triggers excitotoxicity, increases brain free radicals and lipid peroxidation products, inhibits critical brain enzymes, inhibits antioxidant enzymes and impairs DNA repair ability”.
Dr. Boyd Hayley performed a synergy experiment using aluminum hydroxide, mercury & neomycin (antibiotic associated with Kidney Failure, hazardous to a fetus). The results indicated a 75% acceleration in cell deaths when all 3 ingredients were combined.
Thimerosal Mercury in vaccines permanently damages tissue sensitivity – ‘Neonatal administration of a vaccine preservative, thimerosal, produces lasting impairment of nociception (awareness of tissue injury) and apparent activation of opioid system in rats. Present findings show that THIM (Thimerosal) administration to suckling or adult rats impairs sensitivity to pain, apparently due to activation the endogenous opioid system.’
Aluminum + Thimerosal = twice the toxic overload – ‘Mercury readily combines with aluminium to form a mercury-aluminium amalgam when the two pure metals come into contact. A small amount of mercury can “eat through” a large amount of aluminium over time, by progressively forming amalgam and relinquishing the aluminium as oxide.’ Whereas Aluminum is the more dominant metal as a coagulant & in terms of its net charge on the body, Mercury is clearly the more corrosive element.
“A small dose of mercury that kills 1 in 100 rats and a dose of aluminum that will kill 1 in 100 rats, when combined have a striking effect: all the rats die. Doses of mercury that have a 1 percent mortality will have a 100 percent mortality rate if some aluminum is there.” Donald Miller, M.D. Professor of Surgery, University of Washington
See VRM: The Problem With Vaccines Part 2 – Synergistic Effect of Heavy Metal Toxicity On The Body
—————————————————————————————————————–—-
Christmas message from the Vaccine Resistance Movement
IT TAKES COURAGE TO SPEAK THE TRUTH. IT REQUIRES EVEN MORE COURAGE TO LEARN FROM THE MESSAGE GIVEN AND TO TAKE THE NECESSARY STEPS TO TRANSFORM YOUR LIFE ACCORDINGLY
Based on all my research into the mainstream Medical Mafia, I have come away with one prevailing conclusion: The whole foundation on which symptom-based Allopathic Medicine is built runs counter to the holistic principles of the human body, a medieval construct which has been undermining natural immunity since its inception in the early 19th Century; unleashing a cat’s cradle of hybrid cancers on our communities at large. Our children have also become breeding grounds for laboratory produced pathogens, bacterium & rogue, weaponized viruses.
The advent of “Herd Immunity” has done more to damage “natural” immunity than any plague or war experienced through the history of civilization. The entire methodology behind vaccines, including the manufacturing process itself, is rife with problems. We have become nothing more than statistics on a graph, vessels in a multi-billion dollar Industry out of control; one beholden to its own relentless greed. We were never meant to die so young nor suffer the litany of infections, disorders & diseases now plaguing our lives.
The Medical Establishment clearly values profit-making over enhancing the quality & longevity of life. Our Governments have seen fit to broker secret, binding deals with the UN/WHO & Vaccine Manufacturers, to the detriment of our safety & inherent, natural-born rights. We are seemingly headed toward a nightmare scenario, soon to be stripped of our fundamental privilege to choose, to determine for ourselves & our families what goes into our bodies. The only hope is to make it our primary goal to secure forever our sacred rights to self-determination of the body. This will depend on us taking a stand against whichever form of tyranny that threatens these fundamental, natural born, freedoms.
The transition to self-sufficiency, in terms of restoring optimal natural health in the body, requires a genuine paradigm shift in consciousness AWAY from dependency on outside forces, by reclaiming the inherent instinct for survival and unregulated communal living; where-in we can relearn the wisdom & knowledge of natural cures (via tinctures, broths, ointments, spices, essential oils, phytonutrient & antioxidant derived holistic remedies) which our ancestors coveted and passed on from generation to generation within the community.
The path to self-determination of the body MUST be taken alone. In order to discover your own inherent strength of will, the ability to see past all the lies & propaganda that have been foisted upon you and those around you (by those chosen Elites in positions of high power who seek to control you) for generations, you must walk that solo path up the proverbial mountain, to gradually unfurl the damage done to your capacity for natural immunity and genuine unregulated free-will. Only by facing your fears and self-doubt ALONE can you attain that strength within your heart to stand free from tyranny. This is key to self-empowerment. Those who have sought to keep you in bondage since civilization has existed, know this to be true. And they fear your strength, as they turn away from their own capacity for humanity.
I am now convinced that there is but one path out of the mess created by Western Allopathic Medicine and all its hazards & mistakes: Just walk away. What I am advocating is making a clean break, by completely divorcing yourself from all their rhetoric, all the toxic products that are peddled in the name of mainstream medicine, and returning to that sacred path on which our ancestors still stand. Their knowledge is your strength. You certainly won’t regret it. Merry Christmas, one & all, from the Vaccine Resistance Movement

—————————————————————————————————————–—

I find it ironic that my work on vaccines receives the most criticism & scepticism from those mainstream medical professionals (fresh out of Medical school) working on the front lines. The vast majority of parents I encounter, however, particularly those with children suffering from neurological & neurodevelopmental difficulties, are able to grasp the evidence I lay out before them without prejudice; avoiding the trap common amongst those trained in the halls of Western Allopathic Medicine, that of consciously obstructing one’s capacity for critical thinking, when the truth flies in the face of everything you were taught to believe, everything you have invested in.
Typically, graduate level Medical students are the most arrogant in their newfound position & overall understanding of natural health, likewise the most vocal toward those who oppose their ingrained viewpoints; where-as veteran mainstream doctors on the front lines tend to withdraw from all such discussions, avoiding unnecessary controversy, choosing instead to rely on Medical seminar data & the omnipotent Big Pharma supply line to justify their actions visa vi promoting vaccine uptake. VRM
—————————————————————————————————————–—-
In the aftermath of the devastating tragedy in Newtown, Connecticut, this is clearly a time for heart-felt grieving and close family reflection. However, it is still CRITICALLY important to note that the shooter, Adam Lanza, was diagnozed with Asperger Syndrome, a higher functioning form of Autism, which manifests in delayed social & motor skills, plus extreme sensitivity to sensory stimuli (a commonality of symptoms with those children coping with severe forms of Autism ie. identical dietary deficiencies).
The Mayo Clinic routinely recommends the use of anti-depressants & anti-psychotic drugs (Selective Serotonin Re-uptake Inhibitors) for Autism related “symptom management”. It will undoubtedly surface in the coming days & weeks, that Adam Lanza had been prescribed “Antipsychotic medication” such as thioridazine (Mellaril), haloperidol (Haldol), chlorpromazine (Thorazine), clozapine (Clozaril), sertindole (Serlect), olanzapine (Zyprexa), or risperidone (Risperdal), and/or in combination with anti-depressants (Paxil, Prozac, Luvox, Seroxat, Celexa, Lexapro, Cipralex, Zoloft, Lustral, Dilantin, Coumadin) – all of which are ADMITTED to cause psychotic breaks and suicidal-type tendancies in those suggestible/susceptible to inwardly-outwardly destructive thought patterns, particularly in children/teens already close to the edge.
This demonstrates a fundamental lack of understanding of synergistic toxicity, and a clear disconnect between University & Hospital backed Scientific Research divisions and those Medical practitioners working on the front lines – since it has been proven that ALL anti-psychotic drugs have a devastating impact on the Autistic condition, when administered to children to with advanced/severe Autism – linked to a cascading neuro-developmental syndrome known as Tardive Dyskinesia…’characterized by repetitive, involuntary, purposeless movements. Features of the disorder may include grimacing, tongue protrusion, lip smacking, puckering & pursing, rapid eye blinking. Rapid movements of the arms, legs, trunk may also occur.’
In this case, Adam Lanza felt increasingly isolated within his community, despite his mother’s apparent devotion to him, had withdrawn from those capable of addresing his needs on all fronts, and either could not reach out for or refused support, hindered by his Asperger’s condition – which was undoubtedly exaserbated by years of exposure to prescription anti-depressants & anti-psychotic drugs – fed into by a video-game culture which promotes irrational violence and self-loathing. My point is, this individual was not a monster by nature. And the fact that he had access to guns is not the root of the problem. My heart weeps for all these beautiful children and adults whose lives have been cut short so violently. Perhaps now we can dig deeper, to ensure our children aren’t led down the same distorted path, that ultimately love and family will endure and ENSURE that such attrocious acts never see the light of day again. VRM
—————————————————————————————————————–—-