The first legitimate 21st century pandemic has materialized, one which is already proving to be a bona fide threat to humanity, with a stealth chimera pathogen of yet unknown origin moving through the population at an astounding rate. Even in its most intense phase, the 2009 Swine Flu pandemic paled in comparison. According to Tim Trevan, a biological safety expert based in Maryland, “The vast majority of new, nasty diseases…come from nature.” I would preface that statement with a warning. Nature has been usurped by the medical establishment, converted into a giant repository field trial for untested formulae, which has begun to unhinge its delicate balance, giving rise to bizarre chimera pathogens (which never would have surfaced, but for their intervention).
At this stage, it is crucial to evaluate only the facts on the ground. Without a doubt, Covid-19 has emerged as the result of decades of laboratory experimentation with virus technology and vaccines. We do know with certainty that the Wuhan Institute of Virology, which specializes in researching Coronaviruses transmitted by bats, formally conducted intensive studies, making alterations to the SARS-Corona viral template in December, 2015. The level 4 bio-lab is situated adjacent to the market epicenter of the recent outbreak, where a majority of serious cases of Corona were first documented. Researchers working at the Institute were deliberately tampering with the genetic template of the SARS virus or Severe acute respiratory syndrome, passaging the “SHC014” bat strain into mice. The process of synthetic replication of recombinant viruses, by way of a mechanically directed transference of genetic material, in vitro, from one species over into another, poses unlimited, abject risks to human health, given an uncontrolled release, environmental exposure to these unconventional host vectors. But the important unanswered question is, were their workers at the lab exposed to the viral contents, or did any discarded, contaminated material find its way into their water supply, finally ending up in the market, or was it transferred outside unsuspectingly?
Excerpts from the research report reveal an open-ended approach, which integrated bat-mouse genes, triggering haphazard, mutagenic responses, thereby successfully altering the SARS virus into something far more unpredictable, by all accounts, a comparable blueprint for the subsequent Covid-19 strain currently unfolding its fury upon the globe: ‘Using the SARS-CoV reverse genetics system, we generated and characterized a chimeric virus expressing the spike of bat coronavirus SHC014 in a mouse-adapted SARS-CoV backbone. The results indicate that group 2b viruses encoding the SHC014 spike in a wild-type backbone can efficiently use multiple orthologs of the SARS receptor human angiotensin converting enzyme II (ACE2), replicate efficiently in primary human airway cells and achieve in vitro titers equivalent to epidemic strains of SARS-CoV. Additionally, in vivo experiments demonstrate replication of the chimeric virus in mouse lung with notable pathogenesis. Evaluation of available SARS-based immune-therapeutic and prophylactic modalities revealed poor efficacy; both monoclonal antibody and vaccine approaches failed to neutralize and protect from infection with CoVs using the novel spike protein. On the basis of these findings, we synthetically re-derived an infectious full-length SHC014 recombinant virus and demonstrate robust viral replication both in vitro and in vivo. Our work suggests a potential risk of SARS-CoV re-emergence from viruses currently circulating in bat populations.’ The data delineates the earliest stages of a synthetic man-made chimera virus, articulating the precise viral mutations which manifested, derived from SARS RNA. Given the track-record of shoddy protocols, with major laboratory breaches spreading infections documented throughout history, the chances of a genuine “spillover event” having occurred, either by human error, or by way of an intentional leak, conducted with malevolent intent, are high. In the event standard containment measures in the bio-lab interior unit were insufficient; from discarded gloves, gowns and dirty instruments, the altered virus may have been transported inadvertently to the external environment.
“The only impact of this work is the creation, in a lab, of a new, non-natural risk.” Richard Ebright, molecular biologist and biodefence expert at Rutgers University
There is yet another factor to consider. Evidence of SARS virus was detected in the waste matter/feces of victims. This pattern may have been repeated with Covid-19, in a manner reminiscent of SARS. ‘Surprisingly, recent single-cell RNA sequencing data from two independent cohorts revealed a significant enrichment of ACE2 expression in cholangiocytes (59.7% of cells) instead of hepatocytes (2.6% of cells) suggesting that 2019-nCoV might lead to direct damage of intrahepatic bile ducts.’ Staff members and/or cleaners could have become infected, and continued harboring the virus incognito for weeks, as asymptomatic, while virally shedding locally through their stools. Therefore, the urban sewage supply system cannot be ruled out as one potential active reservoir or “hotspot” for this contagion. ‘Before respiratory symptoms, many patients with COVID-19 had diarrhea, nausea, vomiting and abdominal discomfort.‘ For centuries, China has maintained the ancient agricultural tradition – of recycling human waste matter for application as fertilizer, straight into local crops, including the conversion of waste into a source of feed for the people’s food supply: “direct usage as feed for fish.” Corona-contaminated feces is a concern.
- ‘Empirical analysis based on data from stratified random sampling of rural households in five provinces of China shows that about 85% of human excreta was still used as manure in agriculture in 2007 which was less than a decade ago when nearly all human excreta was used as manure…In the case of human excreta, the percentage of human excreta utilized as manure in China was 96% until 1993.‘
- “Importantly, 2019-nCoV has been reported elsewhere in the feces of patients with atypical abdominal symptoms, similar to SARS which was also shed in urine, suggesting a fecal transmission route which is highly transmissible.” William Keevil, a professor of environmental healthcare at the University of Southampton
- “Amounting evidence from former studies of SARS indicated that the gastrointestinal tract (intestine) tropism of SARS coronavirus (SARS-CoV) was verified by the viral detection in biopsy specimens and stool, even in discharged patients, which may partially provide explanations for the gastrointestinal symptoms, potential recurrence and transmission of SARS from persistently shedding human as well.” Jinyang Gu, MD, of the department of transplantation, Xinhua Hospital Affiliated
If the Institute is the original site for this outbreak, the scientific community must apply pressure, demand full disclosure of their activities in the weeks leading up to December 19th, when the index case was reported. In all probability, what we are witnessing is a deliberate cover-up imposed by Chinese authorities, not only on gauging or monitoring the Corona cases, but on the conduct within the Institute. It is almost inconceivable the central Government purposefully green-lighted a leak, unleashed a rogue agent of such destructive force, jeopardizing their hold on the global economy with the express purpose of wiping out a major sector of their own population, without having considered the more serious, far-reaching implications – unless, of course, they didn’t know the true nature of the contagion. This would constitute an act of voluntary terrorism on their nation.
The mystery of Corona is shrouded in international espionage. There were several Chinese nationals caught using false pretenses and stealing lab secrets, in separate incidents, in Canada and United States, which happened shortly before December 19th, 2019, preceding the outbreak. ‘Zaosong Zheng, 30, a Chinese national, was arrested on Dec. 10, 2019, at Boston’s Logan International Airport and charged by criminal complaint with attempting to smuggle 21 vials of biological research to China. On Jan. 21, 2020, Zheng was indicted on one count of smuggling goods from the United States and one count of making false, fictitious or fraudulent statements. He has been detained since Dec. 30, 2019...In August 2018, Zheng entered the United States on a J-1 visa and conducted cancer-cell research at Beth Israel Deaconess Medical Center in Boston from Sept. 4, 2018, to Dec. 9, 2019.‘
Additionally, up in Winnipeg, Canada, a husband and wife team from China are alleged to have absconded with sensitive data from a level 4 bio-lab situated there. Although there has been no official statement made as to a direct connection to the Corona virus, details pertaining to the case are compelling: ‘Dr. Xiangguo Qiu, her husband Keding Cheng and an unknown number of her students from China were removed from Canada’s only level-4 lab on July 5, CBC News has learned. Qiu is a prominent virologist who helped develop ZMapp, a treatment for the deadly Ebola virus which killed more than 11,000 people in West Africa between 2014-2016. She worked with Gary Kobinger, who is now a professor in the Department of Microbiology and Infectious Diseases and director of the Research Centre on Infectious Diseases at Laval University in Quebec.’ While there are few details available, experts say this could be a case of intellectual property theft or technology leakage to China. “The National Microbiology Laboratory would have some pretty sensitive biological research material that could be shared either with or without authorization with foreign countries,” said Gordon Houlden, director of the University of Alberta’s China Institute.’
The most credible evidence presented identifies the Institute in Wuhan as the source. The market is situated only 20 miles from the lab, where a hybrid Corona strain resembling Covid-19 made its beginnings, and had been isolated. Mistakes happen.
In order to gain a foothold on this growing crisis, and its impact on families in the community around the world, it is vital to understand exactly what we’re dealing with. The Coronavirus template is configured somewhat like a Lego set, which can be tweaked and modified with the substitution (either addition or subtraction of individual genes), a molecular biologist’s ideal design prototype. On some level, this strain which has been unleashed is, without a doubt, the product of laboratory alteration, a weaponized, much more virulent version of Corona. I estimate that it has undergone concentrated exposure to multiple species: mammal/avian/reptile, meaning the viral mutation was deliberately passaged via select vectors under the lock-down laboratory conditions, thereby vastly increasing its lethal factor. Covid-19 has been blamed for 7,330 deaths thus far, with 185,067 confirmed “active” cases, 80,237 of which have fully recovered their health. By comparison, the recent SARS outbreak of 2002-04, which culminated in ‘916 deaths at a fatality rate of 11%,’ was merely trail/dry run lead up to Covid-19. Of the 67,799 confirmed cases of Corona in Hubei, China, 56,003 have successfully overcome the virus. While it’s difficult to ascertain an accurate count, given the censorship of information by the Chinese authorities, this drop comes as a sobering thought, indicating the outlying spread is dissipating.
In hindsight, during follow-up analysis into the handling of the SARS epidemic, excessive use of ventilators in intensive care ICU wards was recognized as having contributed to ventilator-associated pneumonia (VAP), and an increase in bacterial contamination. While it is true that extensive sterilization procedures will certainly factor into the dominance of hospital staph infections, chiefly, MRSA, vaccines on the immunization schedule like Prevnar, the Pneumococcal conjugate vaccine PCV are more immediately responsible for seeding an entire generation with the MRSA. Therefore, it is my belief that the SARS infection carried a viral-bacterial hybrid, and that the new Covid-19 sequence contains an underlying bacterial component, Methicillin-resistant Staphylococcus aureus: ‘The MRSA acquisition rate was also increased: it was 3.53% (3.53 cases per 100 admissions) during the pre-SARS period, 25.30% during the SARS period, and 2.21% during the post-SARS period (P<.001). The VAP rate was high, at 36.5 episodes per 1000 ventilator-days, and 47% of episodes were caused by MRSA…There were 30 episodes of VAP in 22 patients, for a rate of 36.5 episodes per 1000 ventilator-days. This is much higher than the 90th percentile distribution for medical ICUs (9.6 episodes per 1000 ventilator-days) or medical-surgical ICUs in major teaching hospital (12.1 per 1000 ventilator-days) in the NNIS system [11]. Most of the organisms causing VAP were MRSA (47.1% of isolates), followed by Stenotrophomonas species (29.4%) and Acinetobacter species (14.7%). During the SARS period, there was a significant increase in the frequency of isolation of MRSA, Stenotrophomonas species, and Candida species and a significant decrease in the frequency of isolation of Pseudomonas and Klebsiella species. There were no differences among the 3 time periods, pre-SARS, SARS, and post-SARS...Infection control measures, in particular, were upgraded, including use of enhanced personal protective equipment (PPE) and more rigorous environment cleansing and disinfection. Infection control measures placed heavy emphasis on use of PPE because of the high rate of transmission of SARS to health care workers. Routinely used PPE included N95 respirators; face shields; caps; long-sleeved, disposable gowns; and gloves. For high-risk procedures, such as intubation and resuscitation, goggles were also used.’ Fast forward to 2020. The same sterilization measures have been carried out in triage units and ICU’s to help combat Covid-19. By extension, MRSA cross-contamination will follow, including the appearance of Mycoplasma, the insidious primitive form of bacterium, which is substantially more pernicious on our heath.
The difficult and unanswered question remains identifying the specific host vectors redistributing the contagion, and essentially getting out of the way of this chimera freight train. The bat theory, which is being touted by experts as the likely source of Corona may in fact be a red herring. A zoonotic origin for SARS has never been confirmed, while the bat reservoir has been speculated as being the primary source.
- “…a specific animal reservoir for the virus has yet to be definitively identified.” Nature Reviews Immunology
- “The origin of its etiological agent, the SARS coronavirus (SARS-CoV), remains elusive.” Science
- “SARS-CoV is thought to be an animal virus from an as-yet-uncertain animal reservoir, perhaps bats, that spread to other animals (civet cats) and first infected humans in the Guangdong province of southern China in 2002.” World Health Organization
The witnessing of Covid-19 virus should be weighed and observed as one would any unnatural hybrid borne of replication, or chemical experimentation and forced exposure to multiple species in a laboratory, isolated from nature: ‘…intermediate hosts are believed to play an important role in the transmission and emergence of these coronaviruses from bats to humans. Understanding the bat origin of human coronaviruses is helpful for the prediction and prevention of another pandemic emergence in the future.’ However, this is not a time for panic but for more clarity.
‘Coronaviruses are enveloped, positive-stranded RNA viruses considered to be promising vectors for vaccine development, as genes can be deleted, resulting in attenuated viruses; their tropism can be modified by manipulation of their spike protein; and heterologous genes can be expressed by simply inserting them with appropriate coronaviral transcription signals into the genome.
Coronaviruses contain a single-stranded, positive-sense RNA genome of about 30 kb, which is capped, polyadenylated, and infectious. All coronaviruses contain a common set of essential genes, of which the open reading frames (ORFs) 1a and 1b, encoding the replicase functions, comprise the first two-thirds of the genome. Downstream therefrom, the essential genes encoding the structural proteins are located, invariably in the order 5′-S-E-M-N-3′. Interspersed between these genes, clusters of group-specific genes occur that are homologous within each group but differ profoundly between the groups. The group-specific genes are accessory genes, as demonstrated by the observed viability of natural and engineered deletion mutants lacking some or all of these genes.
The unique coronavirus transcription mechanism allows the efficient expression of foreign genes simply by inserting these genes together with a TRS into the coronaviral genome, as was demonstrated with several reporter proteins…It is clear, however, that the expression levels of coronavirus genes can be manipulated by changes in the TRS, in the sequences flanking it, or in the position of the gene in the viral genome.‘ TRS: Reference to the ‘transcription regulatory sequences (intergenic sequences) which precede the genes and are homologous to the 3′ end of the leader sequence. The TRSs probably serve as transcription termination or pausing signals, the nascent chain either resuming transcription at the same site or being joined to the leader sequence at the 5′ end during negative-strand synthesis. The negative-strand sgRNAs subsequently function as templates for the production of the positive-strand sgRNA.’ 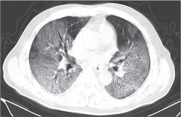
This virus aggressively targets an enzyme in the body called Ace2 or Angiotensin-Converting Enzyme 2, which protects those suffering from hypertension, diabetes, kidney impairment or cardiovascular disease from succumbing to total respiratory collapse. The virus docks onto the enzyme and begins replicating itself, overtaking and inhibiting the respiratory system properties in the process. ‘The virus enters the host cell, and the uncoated genome is transcribed and translated. The mRNAs form a unique “nested set” sharing a common 3′ end. New virions form by budding from host cell membranes.’ The latest configuration of Corona represents a triple weaponized threat: to mature stage adults with pre-existing medical conditions and compromised immunity. It is reminiscent of the T-cell disrupting agent which suddenly manifested in 1978, eventually found to be inserted in the experimental Small Pox vaccine designated for Africa and the Hepatitis B vaccine aimed at the homosexual population in New York and San Francisco. shortly preceding the emergence of HIV Aids. ‘Latest coronavirus research by a team of researchers from Nankai University in Tianjin lead by Professor Ruan Jishou, a prominent virologist and genomicist, have discovered that the new SARS-Cov-2 coronavirus that causes the Covid-19 disease has a mutated gene that is found in HIV virus. It is this unique feature that sets it aside from the rest of the known coronaviruses.’ My inclination here is to suggest that this event is not possibly a natural phenomenon. Covid-19 was unmistakably hatched under laboratory conditions, as the end result of a re-calibrated virus exposed to multiple animal sources, then chemically altered. Like that of Aids and Ebola, this is not a product of nature, or natural selection, but a direct consequence of the forced intervention of man, interrupting and sabotaging the natural life cycle by design. Similar to many mutagenic viruses now in circulation, Covid-19 was entirely avoidable. This pattern will only get worse until we put a halt to licensed medical industry malfeasance.
The striking signature of Covid-19 is a match for HIV. The chances of this occurring in the environment without some form of artificial provocation are virtually nil. ‘We found 4 insertions in the spike glycoprotein (S) which are unique to the 2019-nCoV and are not present in other coronaviruses. Importantly, amino acid residues in all the 4 inserts have identity or similarity to those in the HIV-1 gp120 or HIV-1 Gag. Interestingly, despite the inserts being discontinuous on the primary amino acid sequence, 3D-modelling of the 2019-nCoV suggests that they converge to constitute the receptor binding site. The finding of 4 unique inserts in the 2019-nCoV, all of which have identity /similarity to amino acid residues in key structural proteins of HIV-1 is unlikely to be fortuitous in nature. This work provides yet unknown insights on 2019-nCoV and sheds light on the evolution and pathogenicity of this virus with important implications for diagnosis of this virus.‘ Uncanny similarity of unique inserts in the 2019-nCoV spike protein to HIV-1 gp120 and Gag
Hospital staff have been administering powerful Aids drugs to those stricken to combat the infection. Doctors are basically throwing everything they can at it to slow the spread of condition, with some signs of success. ‘Beijing’s government announced on Sunday that some of the city’s hospitals are giving patients infected with the Wuhan coronavirus medication used to treat HIV, part of efforts to stop the spread of the deadly illness. “Online rumors say that an anti-Aids drug has been used and proved to be effective in treating the coronavirus,” according to a statement by Beijing Municipal Health Commission. “The National Health Commission has recommended the rumored names to treat the coronavirus before and we have Lopinavir/Ritonavir in stock in Beijing,” Three Beijing hospitals designated to treat confirmed coronavirus cases – Beijing Ditan Hospital, Beijing Youan Hospital, and No. 5 Medical Center of PLA General Hospital – have begun using this therapy for treatment, the statement added.’
The RNA-dependent RNA polymerase serves as the skeleton key which latches on the ACE2 enzyme. The trace mineral Zinc ion Zn2+ can effectively halt the viral replication process, potentially saving the life of a patient infected with the Corona virus: ‘Positive-stranded RNA (+RNA) viruses include many important pathogens. They have evolved a variety of replication strategies, but are unified in the fact that an RNA-dependent RNA polymerase (RdRp) functions as the core enzyme of their RNA-synthesizing machinery. The RdRp is commonly embedded in a membrane-associated replication complex that is assembled from viral RNA, and viral and host proteins. Given their crucial function in the viral replicative cycle, RdRps are key targets for antiviral research. Increased intracellular Zn2+ concentrations are known to efficiently impair replication of a number of RNA viruses…by interfering with correct proteolytic processing of viral polyproteins.’ Aids, Ebola and Coronavirus contain an identical T-cell disruptor component. This would be impossible for nature to replicate. It bears the signature of a bio-weapon.
“There is a blueprint, the 1971 research logic of the US Special (HIV) Virus program…a virus that only targets certain persons – as is evidenced by the epidemiology. Here is the final phase, the clinical trials. It was placed in the Small Pox vaccines that went to Africa. Every epidemiology that we have regarding the beginning of HIV & Aids shows that as Small Pox ended, HIV and Aids began in mass in Africa. HIV and Aids began in mass in the late 1970’s as a result of the US Special Virus program and the complementation of that vaccine (refers to the Small Pox vaccine program in Africa) with this special virus (T-Cell disruptor component symptomatic of Aids – authorized by Henry Kissinger) that shows the development of HIV over a period from 1962-1978. How dare you have a Federal Virus program that precedes the greatest onslaught of murder in the history of the world, and you don’t want to acknowledge the program, and you certainly don’t want to review it. The people demand it. This Federal program lies at the heart of HIV and Aids and it needs to be reviewed.” Dr. Boyd Graves – formal testimony given shortly before his premature death
Notably, while numbers are fluctuating daily, ALL of the Corona related deaths being reported show pre-existing medical conditions, and mostly targeting seniors (ranging from 70-80 years +). The Corona scare which is dominating people’s lives is reminiscent of the hysteria surrounding the 2009-10 Swine Flu H1N1 pandemic, fueled by similarly skewed statistics and a media-orchestrated mass hysteria. The death toll being attributed to Corona may not even be accurate, and many of those individuals now being quarantined, labelled as having the virus, could be harboring something else altogether, due to a false-positive diagnosis, common in the heat of a panic-driven crisis. ‘The limitations of molecular testing include the possibility of false-positive results caused by specimen contamination during processing and false-negative results from primer mismatch or inhibitors in the specimen.’
Close to 50% of Corona labelled cases may have been misdiagnosed, merely extreme flu. ‘The multivariate-probabilistic sensitivity analysis results supported the base-case findings, with a 75% probability for the false-positive rate of positive results over 47%. In the close contacts of COVID-19 patients, nearly half or even more of the ‘asymptomatic infected individuals’ reported in the active nucleic acid test screening might be false positives.‘ Potential false-positive rate among the ‘asymptomatic infected individuals’ in close contacts of COVID-19 patients
The SARS outbreak provides a road-map to better understanding and deciphering Covid-19. The mechanism behind it was very similar, albeit the destructive force of this configuration is much greater. ‘We have provided direct evidence that in addition to direct membrane fusion, SARS-CoV can enter cells through an endocytic route, and this endocytic infection leads to viral gene expression. Endocytic entry could expand the cellular range of SARS-CoV, and may explain the replication of SARS-CoV in ACE2-negative colonic enterocytes and liver tissue 37, because macropinocytosis-dependent entry does not require a specific receptor…results also suggest that SARS-CoV is able to enter cells through receptor-mediated, clathrin-independent, caveolae-independent endocytosis, likely through a process involving lipid rafts.’ By all estimates, a large portion of victims categorized as having Corona may have succumbed to bacterial pneumonia, triggered by flu-like symptoms, propelled by a bacterial co-infection, which was documented in 2009-10 during the height of the H1N1 Pandemic. ‘Among 105 children and adults with fatal influenza (US)…7-fold increased risk for invasive methicillin-resistant Staphylococcus Aureus (MRSA).’ Only time will tell whether this runaway virus is an anomaly or a genuine, lasting threat to human survival.
‘The MRSA acquisition rate was also increased: it was 3.53% (3.53 cases per 100 admissions) during the pre-SARS period, 25.30% during the SARS period, and 2.21% during the post-SARS period (P<.001). The VAP rate was high, at 36.5 episodes per 1000 ventilator-days, and 47% of episodes were caused by MRSA…There were 30 episodes of VAP in 22 patients, for a rate of 36.5 episodes per 1000 ventilator-days. This is much higher than the 90th percentile distribution for medical ICUs (9.6 episodes per 1000 ventilator-days) or medical-surgical ICUs in major teaching hospital (12.1 per 1000 ventilator-days) in the NNIS system [11]. Most of the organisms causing VAP were MRSA (47.1% of isolates), followed by Stenotrophomonas species (29.4%) and Acinetobacter species (14.7%).During the SARS period, there was a significant increase in the frequency of isolation of MRSA, Stenotrophomonas species, and Candida species and a significant decrease in the frequency of isolation of Pseudomonas and Klebsiella species. There were no differences among the 3 time periods, pre-SARS, SARS, and post-SARS.’  During the most active SARS phase, doctors in the emergency wards were having considerable difficulty distinguishing between incidence of SARS vs. Mycoplasma pneumoniae pneumonia cases, since SARS and Covid-19 are quite closely aligned. Eventually, we will have gathered sufficient data to determine precisely whether a bacterial co-infection is behind the lethality response seen in the human hosts. I also anticipate a large portion of the deaths are being caused by the intervention of drugs, mainly Tamiflu, as occurred during the Swine Flu pandemic 10 years ago.
During the most active SARS phase, doctors in the emergency wards were having considerable difficulty distinguishing between incidence of SARS vs. Mycoplasma pneumoniae pneumonia cases, since SARS and Covid-19 are quite closely aligned. Eventually, we will have gathered sufficient data to determine precisely whether a bacterial co-infection is behind the lethality response seen in the human hosts. I also anticipate a large portion of the deaths are being caused by the intervention of drugs, mainly Tamiflu, as occurred during the Swine Flu pandemic 10 years ago.
‘75 (76%) patients received antiviral treatment, including oseltamivir (75 mg every 12 h, orally), ganciclovir (0·25 g every 12 h, intravenously), and lopinavir and ritonavir tablets (500 mg twice daily, orally). The duration of antiviral treatment was 3–14 days (median 3 days [IQR 3–6]). Most patients were given antibiotic treatment (table 2); 25 (25%) patients were treated with a single antibiotic and 45 (45%) patients were given combination therapy. The antibiotics used generally covered common pathogens and some atypical pathogens; when secondary bacterial infection occurred, medication was administered according to the results of bacterial culture and drug sensitivity. The antibiotics used were cephalosporins, quinolones, carbapenems, tigecycline against methicillin-resistant Staphylococcus aureus, linezolid, and antifungal drugs. The duration of antibiotic treatment was 3–17 days (median 5 days [IQR 3–7]). 19 (19%) patients were also treated with methylprednisolone sodium succinate, methylprednisolone, and dexamethasone for 3–15 days (median 5 [3–7]). Some patients, especially severely ill ones, had coinfections of bacteria and fungi. Common bacterial cultures of patients with secondary infections included A baumannii, K pneumoniae, A flavus, C glabrata, and C albicans.‘ Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study
What they are not disclosing with accuracy is precisely how many Corona virus cases have stabilized globally. Corona is generating a 2.2% fatality rate, slightly higher in the epicenter China, meaning that hysteria has defined the crisis. Corona virus related deaths have ALL been linked to either 1. Cardiovascular disease; 2. Diabetes; 3. Chronic respiratory disease or 4. Hypertension; including Cancer. Every single victim recorded to date has exhibited some pre-existing medical condition, and there have been zero instances, thus far, of fatality in children and teens. And remember, over twice as many deaths are occurring among aging males. The fatality rate is hovering at 3.4%, however over HALF of the patients in isolation have fully recovered. Many of the deaths being counted may truthfully be presumptive for Corona, so the numbers are still subject to change. The “official” bulletins from the WHO should not be viewed as accurate or complete, as the statistics are in a constant state of flux. ‘Individuals at highest risk for severe disease and death include people aged over 60 years and those with underlying conditions such as hypertension, diabetes, cardiovascular disease, chronic respiratory disease and cancer. Disease in children appears to be relatively rare and mild with approximately 2.4% of the total reported cases reported amongst individuals aged under 19 years. A very small proportion of those aged under 19 years have developed severe (2.5%) or critical disease (0.2%).’
Autopsy report from a middle age man who succumbed to Corona reveal extensive abnormal cellular damage to the lung region marked by acute inflammation. ‘Post-mortem samples from a 50-year old male patient from Wuhan were taken from the lung, liver, and heart. Histological examination showed bilateral diffuse alveolar damage with cellular fibromyxoid exudates. The lung showed evident desquamation of pneumocytes and hyaline membrane formation, indicating acute respiratory distress syndrome (ARDS). Lung tissue also displayed cellular and fibromyxoid exudation, desquamation of pneumocytes and pulmonary oedema. Interstitial mononuclear inflammatory infiltrates, dominated by lymphocytes, were seen in both lungs. Multinucleated syncytial cells with atypical enlarged pneumocytes characterized by large nuclei, amphophilic granular cytoplasm, and prominent nucleoli were identified in the intraalveolar spaces, showing viral cytopathic-like changes. No obvious intranuclear or intracytoplasmic viral inclusions were identified.’

Thankfully, there are immediate natural solutions, safe and efficacious options, to slowing the spread of Corona virus and surviving a prolonged bout of the infection.
(Natural sources include: zinc, melatonin, selenium, VitC/IVC, cysteine, glutathione)
- ‘Here, we not only show that corona- and arterivirus replication can be inhibited by increased Zn2+ levels, but also use both isolated replication complexes and purified recombinant RdRps to demonstrate that this effect may be based on direct inhibition of nidovirus RdRps. The combination of protocols described here will be valuable for future studies into the function of nidoviral enzyme complexes.‘ PLoS Pathogens
- ‘Similar to the analogous human immunodeficiency virus (HIV) and influenza proteins, the S proteins of some coronaviruses—including MHV and the group III coronavirus infectious bronchitis virus—are cleaved into two subunits (S1 and S2) by a cellular protease in virus-producing cells. CD13, the receptor for a number of coronaviruses, is, like ACE2, a zinc metalloprotease.’
- ‘Acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) are clinically severe respiratory disorders, and there are currently no Food and Drug Administration-approved drug therapies. Melatonin is a well-known anti-inflammatory molecule, which has proven to be effective in ALI induced by many conditions. Emerging studies suggest that the NLRP3 inflammasome plays a critical role during ALI. During ALI, the NLRP3 inflammasome is significantly activated with a large amount of IL-1β and the activated caspase-1 occurring in the lung. Melatonin inhibits the activation of the NLRP3 inflammasome by both suppressing the release of extracellular histones and directly blocking histone-induced NLRP3 inflammasome activation. Notably, i.t. route of melatonin administration opens a more efficient therapeutic approach for treating ALI.’
- “Swine flu, bird flu, and SARS, all developed in selenium-deficient China. When patients were given selenium, viral mutation rates dropped and immunity improved.” Dr. Damien Downing, former editor of the Journal of Nutritional and Environmental Medicine
- ‘Recently emerged viral infectious diseases (VIDs) include HIV/AIDS, influenzas H5N1 and 2009 H1N1, SARS, and Ebola hemorrhagic fevers. Earlier research determined metabolic oxidative stress in hosts deficient in antioxidant selenium (Se) (<1 μMol Se/L of blood) induces both impaired human host immunocompetence and rapidly mutated benign variants of RNA viruses to virulence. These viral mutations are consistent, rather than stochastic, and long-lived. When Se-deficient virus-infected hosts were supplemented with dietary Se, viral mutation rates diminished and immunocompetence improved.‘
- ‘We find that the expression of the HIV GPx via a –1 frameshift is enhanced during arginine deficiency, which has been correlated with increased oxidative stress. We have demonstrated an identical heptameric –1 frameshift sequence in the SARS coronavirus, associated with potential Sec codons in the overlapping reading frame, encoding a peptide with significant homology to a family of Se binding proteins. Significantly, serum Se abnormalities have been observed in SARS patients. By this model, the detrimental effects of HIV-1 on the host may be significantly decreased and delayed if optimal Se and sulfur status (cysteine and glutathione) is maintained.’ Selenium and RNA viruses: an update for HIV, SARS, hepatitis and flaviviruses, Prof. Ethan Will Taylor, Ph.D., University of Georgia, Athens, GA
- ‘Lipid enveloped viruses have an evolutionary advantage because their lipid (fatty) coating shields underlying structural proteins from immune surveillance by antibodies. It’s an invisibility cloak; the virus looks mostly like a tiny blob of fat. Some of the more troublesome viruses for human health are lipid enveloped: herpesviruses (all strains), cytomegalovirus (CMV), Epstein-Barr virus (EBV), hepatitis B and C, influenza viruses (all strains, including swine flus and bird flus), Newcastle disease virus, HIV, rubella (German measles), varicella virus (chicken pox), smallpox, swine fever, SARS, West Nile virus and all hemorrhagic viruses (including Ebola). The lipid envelope seriously challenges efforts to make vaccines. Ebola virus and the other hemorrhagic viruses have an added evolutionary advantage: they sequester selenium. The Ebola genome has a repeating sequence of codons that specify selenomethionine incorporation into protein, despite that the virus does not use the resulting selenoprotein directly. It just sits there. The codon sequence is there to deplete the host of selenium reserves so that it cannot mount an effective defense. As it turns out, the oxygen family of elements (oxygen, sulfur and selenium) have antiviral effects against most if not all lipid-enveloped viruses.’
- ‘Dr. Mao stated that his group treated ~50 cases of moderate to severe cases of Covid-19 infection with high dose IVC. The IVC dosing was in the range of 10,000 mg – 20,000 mg a day for 7-10 days, with 10,000 mg for moderate cases and 20,000 for more severe cases, determined by pulmonary status (mostly the oxygenation index) and coagulation status. All patients who received IVC improved and there was no mortality. ‘
Animal rights advocates thinking Coronavirus is nature’s wrath, as a consequence of mankind’s rampant abuse of animals sold for slaughter, need to understand that the same type of brutal exploitation and cross-contamination occurs constantly with vaccine development. The African Green monkey colonies were butchered in the name of scientific advancement, their kidneys appropriated in order to replicate the Poliomavirus for the Polio vaccine. They were harboring a Simian Virus SV40, which was transferred straight into the Polio vaccine, where it still lingers due to a chemical synthesis of the Poliomavirus in 2002. SV40 has left behind a legacy of rarified cancer, including terminal childhood leukemia. Many forms of insidious disease, infection and auto-immune disorders, introduced into the body through vaccines, have permanently altered the human gene pool, including by extensive use of fetal bovine serum derived from cattle, and gelatin derived from pigs, viral vaccine incubators through chickens, dogs, goat and insect viral vectors. Corona is the end product of laboratory experimentation run amok. Human and animal rights have BOTH been trampled on for decades by the vaccine industry, in all fairness.
Government will use the Corona scare as a pretext to fast-track vaccine mandates into law everywhere. We have to be prepared for a series of battles ahead, in the fight for individual health freedom. The most pressing concern on our agenda is an emergency measure decree issued by the World Health Organization, imposed by western leaders upon the community at large, with forced inoculation of the entire population, regardless of quarantines. The plan is in place, all the paperwork ready, awaiting the go ahead (the Model State Emergency Health Powers Act). Buckle up and get out your marching boots, as this is going to be a treacherous year ahead for all of us. Large protest rallies are expected to be springing up around the world.
Thus far, all widespread, non-essential travel restrictions have been recommended, less so imposed – however that is about to change with strict border enforcement; and large public events have been restricted. Thus far, the onus has been placed on families to self-monitor and to self-isolate. But this is a quickly evolving situation. Given the scale of pre-packaged press kit coverage painting a doomsday scenario, the march toward a globally sanctioned forced vaccination policy for every citizen to curtail Corona and “save humanity” is going to be rolled out in unison at an appointed juncture in the coming months. This dilemma has already redefined the landscape, giving rise to new authoritarianism. The WHO was established in 1948 in the wake of fascism, to prevent any repeat of Nazism and secure the foundation and integrity of health rights and freedoms for all nations. Regrettably, powers enshrined to them have been exploited, as Globalism sinks its teeth into humanity. In actuality, the WHO is the hydra protecting and facilitating powerful vaccine corporations, which is a dangerous combination. It is time for families to wake up to uncloaking of the new world order in its glory. We cannot remain passive to this threat, and perhaps the Corona outbreak is the spark that we needed to galvanize and take back what is in the process of being seized from us all, universal, inalienable self-determination of the body, a tenet which was enshrined in the Nuremberg code, which is destined to be shredded and rewritten, unless we intervene.
During a declared Health Emergency ALL individual rights and freedoms enshrined in the Bill of Rights or the Constitution are suspended. The 194 signatory nations united under the “pandemic preparedness” banner have devised formal legislation, which is waiting to be implemented. Governments can assert “legal authority” to force-vaccinate ANYONE for the entire period extending the duration of the WHO’s official declaration of a Pandemic. Nations will have anywhere between 3 months and 1 year to carry out these unlawful, flagrantly unconstitutional orders, depending on the color of law affixed to their specific mandate, and there is absolutely nothing a family wanting to opt out can do but to submit, given the probability that the police and army personnel are going to be accompanying nurses door-to-door during their community-wide sweep.
Forced vaccination will not only cause riots but I fear violence in the streets. Families will be faced with difficult choices when compelled to submit by the point of the gun. As a community, we must ensure that never happens. I suspect these draconian organized crackdowns on health freedom will become a permanent reality. The establishment will never turn back the clock after getting their way. If families roll over to this threat we’re finished, at least we’ll either be arrested or forced to go into hiding. This is the foreseen nightmare scenario I was hoping we could avoid. But I think they’re really going through the steps in a script that was written decades ago in the lead-up to 2020. You can’t quarantine the truth. Apart from the suffering incurred by those people hit hardest by the Corona virus, a monumental tragedy, this year will be remembered as the single, largest social engineering experiment ever conducted on the population in history.
I have been accused, in part, for fueling fear by raising the alarm that imminent forced vaccination may be coming. However, every indicator points to this likelihood. Major governments around the world have just imposed national states of emergency protocols, which legally entitles them to impose forced vaccination on the entire population. This crisis is driven especially by psychological momentum, fomented through a media blitz of ominous “facts and figures” which characterize the global threat posed by the Coronavirus as unprecedented, one which demands complete societal cooperation, otherwise millions of people will die. At no time have the media provided a balance report on the data, the fact that, as of March 16th, 56,003 of the 67,799 Corona cases in Hubei, China, the original epicenter of the outbreak have FULLY recovered. What this means is, the virus may have already peaked, stabilized, and that many of the prognostications on it, have been exaggerated.
The narrative coming out of the World Health Organization, and the wartime pitch being portrayed through the news channels, has families convinced we are in the midst of a silent killer. But the fact is, upwards of 70-80% of those cases being counted as Corona positive may actually be false-positive. Also, many cases being characterized as presumptive for Corona, have turned out to be nothing more than a bad cough or cold masquerading as Corona. Families have been instructed to self-isolate, and social distancing has become the new normal. The stringent restrictions to daily life, job loss, immense personal sacrifice in the name of the greater good has already shifted the community from a mindset of embracing to cautious. When the experimental Corona vaccine is ready, many of those families now shuttered in their homes, will see the option as a relief, and will gladly roll up their sleeve for it. Those families who are unwilling will be ostracized to a degree not experienced since WW2.
The temptation to authorize sweeping vaccine policy on all citizens will be extremely high, and this will be encouraged by the CDC and the WHO. We must be ready for that scenario. If the virus spread is not successfully contained in the coming months, look for geographic indicators, like military checkpoints in urban centers, and media saturation introducing the vaccine as safe and effective. According to Dr. Lisa Jackson, the Kaiser Permanente study leader behind a Corona vaccine prototype, “We don’t know whether this vaccine will induce an immune response, or whether it will be safe.” Dr Peter Hotez, dean of the National School of Tropical Medicine at Baylor College of Medicine, who worked on the SARS vaccine, and ‘found that some vaccinated animals developed more severe disease compared with unvaccinated animals when they were exposed to the virus‘ has gone so far as to say, “I understand the importance of accelerating timelines for vaccines in general, but from everything I know, this is not the vaccine to be doing it with. There is a risk of immune enhancement. The way you reduce that risk is first you show it does not occur in laboratory animals.” This strategy led to Pulmonary Immunopathology in SARS vaccinated mice, in effect creating the condition in healthy mice, worsening any existing mitigating factors, thereby hastening the incidence of an adverse respiratory response. It neither right nor prudent to force a rushed, potentially dangerous product on families which has not been tested on animals, making it a real-time human trial without a safety net for recipients.
We, the ordinary people, are the actual leaders in the community, not our government, and not so-called health experts. It is never wise to defer you personal decisions to an external authority, but especially now. The Corona vaccine is supposed to take at least 12-14 months for clinical trials. At this stage, given the unprecedented scale of the rhetoric we’re hearing it will be fast-tracked into circulation in half the time needed for minimally adequate safety testing. Many people will fall victim to fear-mongering and the general state of panic, and willingly roll up their sleeve to end the ongoing cycle of lock-down, believing the shot is needed in order to stay alive. The global community is being psychologically primed to accept a potentially dangerous vaccine with unknown variables and blind consequences. Expect a widespread surge in cases of Corona due to viral shedding when the vaccine is officially released. We are being lured into mass obedience training for humanity motivated with a cattle prod. Corona is going to be labelled a “perpetual pandemic.”
I can’t stress enough the urgency, as we’re at the headwaters right now of imminent forced vaccination. I say this with absolutely no reservation or doubt. Everyone who is concerned about civil liberties and health freedom, please get active with this issue now. Notify your friends and loved ones. This is the real takeover. It’s happening now. It will unfold far quicker than ever expected. Knowledge is the antidote to fear, and in this hour of need, families have a clear-cut choice: either to remain passive and join the herd or stand free from tyranny. Our ancestors knew which decision to make, because they, too, sensed danger and saw the writing on the wall. Mayday, mayday, mayday!