
The Zika Virus (an RNA virus containing 10,794 nucleotides encoding 3,419 amino acids) has long been considered a relatively innocuous, albeit contagious, localized pathogen, typically producing Flu-like symptoms in the host, on average subsiding within one to two weeks; certainly nothing on the scale comparatively, to that of the Dengue or Yellow Fever Virus variety, let alone Ebola – each of which are associated with varying degrees of internal “blackish” bruising & widespread hemorrhaging (‘gastrointestinal bleeding, haematuria, skin petechiae, ecchymoses’) followed by rapid systemic deterioration, marked by Kidney failure, often leading to death.
‘Most reports describe a self-limiting febrile illness that could easily be mistaken for another arboviral infection, such as dengue or chikungunya fever.` National Institutes of Health

How does this specific vulnerability to vaccines correlate with pregnant women?
Mother & child share the same immunity while the baby is ‘In Utero’ (all 3 trimesters); including the entire duration of breast-feeding after birth. The Placenta and breast milk (Colostrum) are inextricably linked, providing a baby’s primary initial source of nourishment through the long journey of formation in utero – while supplying the basic building blocks of life necessary to guarantee a safe transition into early childhood development.
Via this intrinsic lifeline, the fetus is also rendered highly susceptible to what are termed ‘endogenous retroviruses’ (remnants of ancestral exogenous retroviral infections fixed in the germ-line DNA), passed on inter-generationally – primarily the result of previous exposure (grand-parent to parent to offspring) to the Polio, Tdap & MMR vaccines, from the mid 1950’s through the late 1960’s. The infant inherits any repository of cross-contaminated residue found in these shots, left embedded in the organs, bound to genetic material.
It goes without saying that pregnant women are at a heightened risk of adverse reactions to vaccines.
Granted, any widespread immunization campaign targeting pregnant women which correlates with the epicenter of a sudden surge (mainly throughout sectors of north-eastern Brazil) is highly suspicious, given the verifiable track-record of serious adverse (auto-immune) reactions, neurological trauma and neuro-developmental difficulties, occurring in babies and young children following vaccination with Tdap.
Surprisingly, in this instance, the timeline simply doesn’t match up. Here is why.
First of all, the Tdap vaccine was not strictly enforced as a preventative measure for pregnant women, the key word being “recommended”. Hence, the statistical numbers of those vaccinated women in this community cannot be fully verified.
More importantly, microcephaly has a unique signature which rules out any damage done beyond the second trimester.
The brain and skull cavity develop throughout the first and second trimester. By 24 weeks gestation (in utero), the overall structure, mass & density of both areas has been firmly established.
By the 10th week of pregnancy, or eight weeks after conception, your baby’s head has become more round.’ Mayo Clinic
Beyond that crucial second trimester window, any damage incurred there-after, ie. during the third trimester (from 27-38 weeks) will inevitably hinder early childhood development, but it cannot alter the basic physiology (proportions) of the brain & skull.
‘The most critical period for malformations and disruptions is the third to eighth week of gestation, during which the brain and most organs take form.‘ Dimitri P. Agamanolis M.D.
‘It has been reported that in severe microcephaly the intracranial contents may not be visible sonographically, but this occurs only when the head is extremely small…The available experience suggests that even expert ultrasound in pregnancies at risk will fail to diagnose fetal microcephaly in many cases. As most microcephalic infants have different types of cerebral maldevelopment, attention should be focused not only on the cranial measurements but on the cerebral anatomy as well.‘ Visual Encyclopedia of Ultrasound in Obstetrics and Gynecology
The Tdap vaccine is being administered to pregnant women during the third trimester only. Therefore, based on these discrepancies, it must be ruled out of our investigation.
‘To maximize the maternal antibody response and passive antibody transfer to the infant, optimal timing for Tdap administration is between 27 and 36 weeks gestation (third trimester).‘ Centers for Disease Control (CDC)
‘Maternal immunization during the third trimester, immunization of other infant contacts, and reimmunization during subsequent pregnancies may be necessary.‘ Infectious Disease Society of America, 02/2013
Another red flag indicator of overlapping contradictions, those pregnant women who have given birth to babies with microcephaly, including their male counterpart in many instances, have traces of Zika virus showing up in their blood (male & female), semen (male) and breast milk (female).
‘Virus in blood, semen, milk in Brazil. 3 Dec 2015. FIOCRUZ detected presence of Zika virus in blood, semen and breast milk as announced by The Vice Director of Clinical Services of the National Institute of Infectious Diseases, Jose Serbino Neto.‘ International Society for Infectious Diseases
This shifts the spotlight away from conventional vaccines, in identifying the key determining factor, toward another, more insidious source.
The only other rational, scientific-based explanation implicates mosquitos infected with the Zika Virus. And that is precisely where the primary evidence is pointing.

The male variety of the Aedes aegypti mosquito, importantly, does not transmit disease directly to humans. His role is exclusively to mate with the female mosquito, impregnating as many as five at a time during his short lifespan, until he dies; typically after seven to eight days.
The female (ectoparasite), physically larger in size, is designed solely to reproduce, and, in order to ensure the survival of her eggs, upwards of one to two hundred per batch, must acquire foreign blood, extracted from a mammalian (human) host, with which to see them through to “maturity”.
‘The reason that (female) mosquitoes need to feed on our blood (containing proteins) is to reproduce. So the way that they find us is through olfaction (sense of odor/smell). When mosquitos find us (via the carbon dioxide plume we emit) and bite us, or blood-feed from us, that is when they transmit infectious disease agents. So if we can prevent mosquitos from finding us, then we can prevent transmission of the diseases.‘ National Institute for Allergy & Infectious Diseases
What is the vital connection between the Zika Virus contagion, the Aedes aegypti Mosquito, and ensuing cases of Microcephaly? Until now, the answers have been shrouded in conjecture, false leads and unsubstantiated data.
Back in 2011, when I completed ‘VRM: The Problem With Vaccines Part 3 – Synthetic Genomics & The Death Of Natural Immunity’, synthetic biology was still in its infancy.
The writing was on the wall, even then, sounding the alarm, as to the imminent risks posed by tampering with nature’s delicate infrastructure, the imposition of transgenic organisms on a naturally evolving wild species.
Cutting edge, fly-by-night corporations are positioned to capitalize on a “wild west” of radical technological experimentation. Much like the corrupt vaccine industry, these white-collar criminal enterprises are also exempt from liability, or accountability.
We are told they are rendering a great service to society, the absence of which, our communities would be left at the mercy of nature`s cruel hand. But who is actually gambling with our lives here? Nature is not your adversary.
Benefits and risks extend to humans, nonhuman species, and the environment, each with unique needs and vulnerabilities. Emerging technologies present particularly profound challenges for responsible stewardship because our understanding of these potential benefits and risks is largely incomplete, preliminary, and uncertain. The prospect of intentional misuse by malicious actors further complicates efforts to respond adequately to the spectrum of benefits and risks.’ The Ethics of Synthetic Biology and Emerging Technologies/Presidential Commission for the Study of Bioethical Issues, Washington, D.C., 2010
‘Some have advocated a total precautionary principle for genetic engineering, which means that no technology with any known risk should be attempted…Since no human action can be guaranteed to have zero risk, in practice, these principles are used to assess the relative safety of technology and are central to any public health program.‘ Discussion on the proposed hypothetical risks in relation to open field release of a self-limiting transgenic Aedes aegypti mosquito strains to combat dengue, Molecular Biotechnology, 05/05/2010
Fast forward to 2016. Brazil is currently ground zero for the most ambitious, cross-species genetic engineering experiment ever conducted on a human demographic.
Financed primarily with the support of a ‘$19.7 million grant from the Bill & Melinda Gates Foundation‘ Oxitec, a subsidiary of Intrexon Corporation, a leader in synthetic biology, quietly began testing a genetically engineered (GE) prototype mosquito, under the radar, as early as 2009.
‘Oxitec’s mosquito, locally known as ‘Friendly Aedes aegypti’, is a revolutionary and environmentally sustainable tool that has already shown suppression of infestations of the wild Aedes aegypti mosquito, a goal which we’ve been trying to achieve for many years in Brazil but haven’t been able to. This solution is even more important today because beyond the dengue epidemic, we now have the Zika virus and chikungunya in Brazil,”, said Professor Wagner Pereira from Veiga de Almeida University.‘

Despite bold predictions of success, and a relentless campaign endorsing the GE mosquito from Government Health departments, backed by mainstream media outlets, it was clear from the start that safety protocols had been bypassed altogether, legitimate field trial data white-washed and exaggerated, in an attempt to fast-track their technology into commercial production.
Take note of the date, May 15, 2014, which marked the start of a widespread release of transgenic mosquitoes into the environment.
Officially, field trials involving GE Mosquitos began in June of 2013, in the State of Bahia, Brazil; where two Microcephaly-related deaths were later reported (December 2015).
‘The CTNBio (Brazil’s National Technical Commission for Biosecurity) set a dangerous precedent by approving the commercial release of the (GE) mosquitoes before full epidemiological studies had been completed.’ Leonardo Melgarejo, Brazilian Ministry of Agrarian Development, and economist Antonio Inacio Andrioli, Regional Northwest University of Rio Grande do Sul in Brazil
“It is extraordinary that experiments with Oxitec’s GM mosquitoes continue and commercial releases have even been approved without any monitoring of the effect on dengue.” Dr Helen Wallace, Director of GeneWatch UK
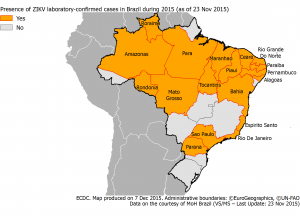
The first cluster of confirmed cases of Zika Virus in the epicenter region of Northeastern Brazil (Rio Grande do Norte) occurred in the early Spring of 2015.
The index (first recorded) case in Brazil involving Zika Virus concomitantly with Microcephaly surfaced in November of 2015, in the State of Paraiba, which borders that of Rio Grande do Norte.
Both pregnant women presented compatible symptoms of ZIKV infection during their pregnancy.
Based on the temporal correlation of these cases with the Zika epidemic, the health authorities of French Polynesia hypothesise that ZIKV infection may be associated with these abnormalities if mothers are infected during the first or second trimester of pregnancy.‘ European Centre for Disease Prevention and Control, 11/24/2015
Logically, the mothers-to-be, in this instance, would have had to conceive by March of 2015, to given birth to their babies in November of the same year – ample opportunity for early (first trimester) exposure to the GE mosquito.
Note: ‘25 million transgenic insects were released between April and November‘ of 2015.
Why was Oxitec so determined to avoid formal scrutiny? What were they hiding?
It turns out the formula behind the GE Mosquito, OX513A, requires the use of an antibiotic, tetracycline hydrochloride (Sigma®): ‘Add a stock solution of tetracycline (3 mg/ml in water – microgram per milliliter (µg/ml)) to the trays at a 1:100 dilution to obtain the required final concentration of 30 µg/ml.‘
Oxitec’s “conditional lethality” trait is created by genetically engineering the mosquitos to express a protein called tTA (tetracycline-controlled transactivator). High level expression of tTA is toxic to the mosquitos and kills them at the larval stage, although the mechanism for this is not fully understood.‘ Scientist Helen Wallace, Director of GeneWatch UK, excerpt from – Genetically Modified Mosquitoes: Ongoing Concerns
The goal is to outnumber & outsmart the natural selection process in the Aedes aegypti Mosquito population, whereby the laboratory altered male will successfully mate with the wild female, and pass on the sterilizing tetracycline agent; to neutralize, ie. ensure the termination, of any offfspring (eggs).
“At the end of the day, It’s a numbers game. The more mosquitoes are out there, the more we release. We just need to outnumber the (wild) males….Each one of the (GE) males we release, die.” Oxitec CEO Hadyn Parry
The antibiotic is expected to sustain the GE male mosquito just long enough to procreate. He then embeds the antibiotic protein tTA into the wild female, and apparently dies off thereafter. Any offspring, deprived of Tetracycline at birth, will not survive past the larval stage of development – an altogether expensive & reckless theory, which has been vigorously challenged by numerous genetic engineering watchdog groups for its questionable scientific merits.
‘Oxitec has made misleading statements repeatedly in the media that its GM mosquitoes are sterile.‘ GeneWatch UK Briefing, December 2010


On its face, 30 µg/ml (micrograms per millilitre) of tetracycline may not raise concern. After all, the product has been widely used on the market for decades, administered to treat acne and other bacterial infections; including applications in industrial agriculture.
This prescription antibiotic is strictly meant to be taken orally, ‘comes as a capsule and suspension (liquid) to take by mouth’, and is only ever injected for Veterinary purposes (mainly cattle & horses).

A pregnant woman is highly vulnerable to drugs & antibiotics, particularly throughout the first trimester. Any minimal exposure is enough to seriously damage the fetus.
‘Tetracyclines have been shown to cross the placenta and may affect fetal bone formation‘
‘Tetracycline has been assigned to pregnancy category D by the FDA. Animal studies have revealed evidence of embryotoxicity (a substance that crosses the placental barrier; Injury to the embryo, which may result in death, growth retardation, or abnormal development of a part that may affect either its structure or function) and teratogenicity (developmental malformations) ie. birth defects, including toxic effects on skeletal formation.’
Growth retardation, abnormal development, congenital defects, developmental malformations, toxic effects on skeletal formation, evidence of embryotoxicity: these are all textbook definitions of Microcephaly. Without a doubt, we have found our culprit. The clinical evidence is overwhelming.
Precisely how is tetracycline getting into the bloodstream of pregnant women?
Female mosquitoes are essentially the equivalent of flying vaccinators. The transgenic male, saturated in tetracycline solution, goes on to impregnate the wild female, cross-contaminating her system with the antibiotic, where-upon she transfers the toxic serum into the blood-stream of the awaiting human host; in this case, pregnant women.
Millions of voracious transgenic mosquitos are on the loose, jeopardizing the safety of any pregnant woman, from exposure to multiple numbers of (cross-contaminated) female mosquito bites.
It doesn’t require a PhD in mathematics to recognize an imminent threat posed by this situation, if left unchecked – the accumulative effect, on fetal development, from prolonged tetracycline build-up in the bloodstream. For thousands of families, the real damage has already been done, and cannot be reversed.
Disturbingly, the synergistic effect of this unnatural collision of nature & technology has the potential to heighten the blood-seeking behavior of the female, including her ability to readily transmit the Zika Virus: ‘Potential hazard SI No. (5): Wild females become aggressive after mating with GE sterile males. Increased biting activities (bloodmeal feasting on humans) and increased disease transmission (Zika Virus).‘
The long-term implications, in terms of the environmental impact, of introducing a laboratory-produced hybrid form of mosquito into an already fragile ecosystem, are unknown.
The long-term implications, in terms of the human cost, from a novel epidemic of this kind, impacting and altering our communities, are being completely ignored by health “authorities”.
The immediate consequences have been nothing short of disastrous.
Figures being reported are fluctuating daily, not surprisingly, given the general state of panic surrounding a crisis of this magnitude. The Zika Virus scare could turn out to be another overblown Pandemic, as we endured back in 2009. It could also be far more serious than we recognize at this stage. Caution and preparedness for any contingency are absolutely necessary.
One of the main reasons why statistical estimates on the number of cases of microcephaly have dropped, the criterion has recently been redefined. Many of those babies previously registered as having Microcephaly, showing a lesser reduction (circumference) in cranial size, have since been discounted.
‘As of 4 Dec 2015, the Brazil Ministry of Health has changed the criterion of microcephaly from 33 cm head circumference to 32 cm. This is expected to reduce the microcephaly case numbers considerably.‘
‘I am now declaring that the recent cluster of microcephaly cases and other neurological disorders reported in Brazil, following a similar cluster in French Polynesia in 2014, constitutes a Public Health Emergency of International Concern.‘ WHO Director-General summarizes the outcome of the Emergency Committee on Zika, 02/01/2016

A team of doctors from the Faculty of Medicine, University of Buenos Aires, Argentina, have challenged the GE mosquito-Zika Virus-Microcephaly connection. They allege the use of a chemical larvicide, Pyroproxyfen, in high-density areas, is singularly to blame for the spike in cases of microcephaly.
Field trials involving the larvicide, pyriproxyfen, currently being used to combat the Aedes aegypti mosquito population in Brazil, were conducted extensively during 2005-2006, in several concentrated regions (Malaysia. Peru & Cambodia).
A variation of same product has been used for decades in California and elsewhere, as an environmental insecticide, to mitigate loss in crop production.
If pyriproxyfen was responsible for the sudden unprecedented surge in cases of microcephaly on the ground in Brazil, then why did we not see similar outbreaks or clusters previously in Malaysia. Peru & Cambodia, let alone California?
There is already verifiable evidence linking the use of the antibiotic, tetracycline, as a sterilizing agent on Genetically Engineered mosquitos, with congenital malformations (teratogenicity).
There is no association between the application of pyriproxyfen in reservoirs, and the presence of the Zika Virus infection in the blood, semen & breast milk of many of those couples whose child was born with microcephaly.
Clearly, pyriproxyfen is a toxic substance that has irrevocably harmed the environment. However, speculation linking pyriproxyfen with Microcephaly is nothing short of speculative at this stage, because a connection cannot be verified without proper laboratory analysis – requiring blood samples taken from those women living in concentrated areas affected; whose child was born with birth defects.
There is a plausible argument for cross-contamination of the reservoirs, supplying impoverished communities in north-eastern Brazil, compounded by the Aedes aegypti mosquito. Could pregnant women absorb enough pyriproxyfen to seriously damage the fetus? Without further testing and medical verification of concomitant factors, on a case-by-case basis, any such hypothesis must remain inconclusive. This reinforces and confirms tetracycline as the main causal agent.

The genie is out of the bottle. Genetic engineering has unfortunately arrived, and begun to challenge nature in ways that no scientific analysis can determine. One thing is for certain, nature has proven, throughout history, a capacity to rebound against man’s interventions. Rest assured, nature will respond to man’s attempts at reshuffling the deck by literally re-assorting humankind.
We are witnessing the early stages of a nightmare scenario, unfolding before our eyes. This is a live field trial being conducted in real time, on an unsuspecting population. The problem now is, you can’t turn back the clock.
Millions of genetically engineered mosquitoes have already been released into the local environment, rendering any nation vulnerable to similar outbreaks on their own soil.
The survivability or adaptability of the GE mosquito, how its biochemistry reacts with other species, or replicates and spreads circulating viruses & bacterium, will ultimately depend on a myriad of unpredictable factors.

A researcher at Rockefeller University feeds her stock of yellow fever mosquitoes.
The stakes are high in Brazil, given the limitations posed by economic disparity in isolated rural communities, the fall-out from decades of Industrial waste, polluting of the soil & water-ways, coupled with insufficient hygiene, sanitation standards & nutrition brought on by poverty – a resulting dependency on and vulnerability toward government & World Health Organization sanctioned Health directives.
This is irrefutably a major crime against humanity. And yet, corporate malfeasance of this magnitude is commonplace in the Medical Industry, similar in scale to the watershed Thalidomide scandal of the 1960’s, yet far more concerning from a human perspective, given the potential for mutagenic shifts in viruses & bacterium exposed to transgenic technology, toward a far more virulent “weaponized” type of strain.
Eventually, corporations such as Oxitec are held accountable for their gross misconduct, as countless families, impacted by these reckless, profit-making schemes, band together as one, organize class action lawsuits, and speak out in public. Financial liability simply doesn’t constitute justice served, given the suffering incurred within these families.
Beyond the devastating daily reality posed by Microcephaly, as innocent children are being stripped of a normal life at birth, there is a hidden legacy of social stigma and inward shame many parents will have to endure in silence.
Families are fed up. Something has to be done now to stop this cycle of abuse. It is our responsibility as concerned citizens, proactive parents and critically- thinking individuals, to become educated on these clear and present dangers to our health, to encourage safe, viable alternatives to western Allopathic methods & Medical Industry propaganda, and to resist government wrong-doings without fear of retribution.
After all, elected representatives green-lighted nothing short of a Frankenstein experiment on their own people, without any oversight or precautionary measures; and have thus, inadvertently placed the health & safety of the entire global community at risk.
Given enough resources, this misguided Industry will eventually have the ability, and the authority, to re-engineer our entire species, in fact, any species, at will. The whole issue of genetic engineering, the immersion of transgenic organisms into the environment, needs to be front & center on the political radar. We don’t have a generation to observe the results. It’s time to take a stand now, to do your share, while we still can, and make an impact on humanity’s course of action.
Ask yourself, where has our systemic, blind faith in outside forces gotten us thus far? The question is, what are you prepared to do about it? Fortunately, the solution is within your reach. Knowledge is much stronger than tyranny. And in the end, the truth is stronger than lies. Our children deserve the right to a brighter future, and we must, accordingly, lead by example.
See: VRM: Ebola Report
See: VRM: Measles Report
See: VRM: Vaccines Do Contain Aborted Human Fetal Tissue
See: VRM: The Rise of Mutagenic Viruses
VRM: The Autism Report http://vaccineresistancemovement.org/?p=10185
VRM: Worldwide Autism Study Direct link to study: http://study.vaccineresistancemovement.org/
VRM: The Problem With Vaccines Part 1 http://vaccineresistancemovement.org/?p=488
VRM: Vaccine Clinic – A Concise Compendium To The Problem With Vaccineshttp://vaccineresistancemovement.org/?p=6278
VRM: The Problem With Vaccines Part 2 – Synergistic Effect of Heavy Metal Toxicity On The Body http://vaccineresistancemovement.org/?p=6097
VRM: The Problem With Vaccines Part 3 – Synthetic Genomics & The Death Of Natural Immunity http://vaccineresistancemovement.org/?p=6880
VRM: A Concise Compendium To The Problem With Vaccines Part 3 – Synthetic Genomics & The Death Of Natural Immunity http://vaccineresistancemovement.org/?p=7283
VRM: The Problem With Vaccines Part 4 – Primary Aspects of Vaccine Toxicity Affecting Body http://vaccineresistancemovement.org/?p=8787
VRM: The Problem With Vaccines Part 5A – Detoxification & Restoration of the Body http://vaccineresistancemovement.org/?p=8836
VRM: The Problem With Vaccines Part 5B – Detoxification & Restoration of the Body http://vaccineresistancemovement.org/?p=8847
VRM: PCV Vaccine Exposed – Breeding Ground For Staphylococcus Aureus http://vaccineresistancemovement.org/?p=9431
VRM: Pandemic Preparedness & The Dark Agenda Ahead http://vaccineresistancemovement.org/?p=9460
VRM: Polio – United Nations & The Great Cull http://vaccineresistancemovement.org/?p=4916
VRM: The Re-emergence of Polio in The Third World (compliments of the World Health Organization & Bill Gates) http://vaccineresistancemovement.org/?p=10091
VRM: Weaponized Polio & The African Green Monkey Conundrum http://vaccineresistancemovement.org/?p=10727
VRM: Mandatory Vaccinations – How They Will Be Implemented http://vaccineresistancemovement.org/?p=11806
VRM: The Confidential Case-files of GlaxoSmithKline – Cover-up, Deferral & Denial of Responsibility for Vaccine-related Premature Deaths http://vaccineresistancemovement.org/?p=12242
VRM: Primary Reasons Not To Get The Flu Shot http://vaccineresistancemovement.org/?p=12642
VRM: The Flu Report http://vaccineresistancemovement.org/?p=9226
VRM: Vaccine Ingredients http://vaccineresistancemovement.org/?p=979
VRM: Safe Alternatives to Vaccineshttp://vaccineresistancemovement.org/?p=662%EF%BB%BF
VRM: Family Charts Gradual Decline Of Daughter http://vaccineresistancemovement.org/?p=3156
VRM: Health Matters Part 1 http://vaccineresistancemovement.org/?p=6719
VRM: Health Matters Part 2http://vaccineresistancemovement.org/?p=6746%EF%BB%BF
VRM: Alternative Cancer Cures That Work http://vaccineresistancemovement.org/?p=3729
VRM: Pregnancy Tipshttp://vaccineresistancemovement.org/?p=3270
VRM: H1N1 Shot Reactions – Miscarriages http://vaccineresistancemovement.org/?p=943
VRM: The Vanishing Sperm Count http://vaccineresistancemovement.org/?p=4639
VRM: H1N1 Vaccine Surplus From 2009 Reveals Growing Distrust of Gov’t & WHO http://vaccineresistancemovement.org/?p=4969
VRM: Flu Death Statistics – WHO & The Big Lie http://vaccineresistancemovement.org/?p=784
VRM: Vaccine Industry Deception, Propaganda & Media Collusionhttp://vaccineresistancemovement.org/?p=197
VRM: Birth of Medical & Scientific Dictatorship – Future Scenarios http://vaccineresistancemovement.org/?p=997
VRM: H1N1 Bio-weaponry Incorporated http://vaccineresistancemovement.org/?p=884
VRM: Aids & The WHO Connection – Criminal Intenthttp://vaccineresistancemovement.org/?p=1749
VRM: Morgellons Syndrome & Chemtrails http://vaccineresistancemovement.org/?p=839
VRM: Council On Foreign Relations 10/16/09- Major Influence on Government Vaccine Policyhttp://vaccineresistancemovement.org/?p=1880
VRM: Closed Door CDC Meeting Reveals Industry Cover-up Of Heavy Metal Toxicity In Vaccines http://vaccineresistancemovement.org/?p=5935
VRM: The Rockefeller Foundation Drafts A Post-Pandemic Scenario http://vaccineresistancemovement.org/?p=5102
VRM: World Health Organization & Vaccine Manufacturers Implicated In Massive H1N1 Financial Scam Involving Kickbacks & Cover-upshttp://vaccineresistancemovement.org/?p=4610
VRM Live – 01/28/11: Vaccine Resistance Movement founder Joel Lord discusses Synthetic Genomics, cloned cell vaccine technology & the death of natural immunity, gutter journalism & Dr. Wakefield’s imminent vindication with ‘Truth to Power’ host Paul Mabelis. http://www.blogtalkradio.com/empradio/2011/01/28/truth-to-power-thursday
VRM Live – 11/04/10: Vaccine Resistance Movement founder Joel Lord lays out the whole vaccine process with Paul Mabelis; including heavy metal toxicity, synergy, pregnancy issues & the basic principles of natural health at risk. http://www.blogtalkradio.com/show.aspx?userurl=empradio&year=2010&month=11&day=05&url=truth-to-power-thursday
VRM Live – 09/24/10: Vaccine Resistance Movement Founder Joel Lord & activist/radio host Jesse Calhoun lay it all out tonite. Topics include the VRM Worldwide Autism Study, Scientific/Medical dictatorship, Natural Rights & Vaccine Industry fraud exposed. Special thanks to host Paul Mabelis. http://www.blogtalkradio.com/empradio/2010/09/24/truth-to-power-thursday
If you appreciate the efforts to bring this information forward do consider making a donation. Any amount, no matter how small will help enable me to carry on this invaluable research. See Paypal link on the VRM website (click on ‘Donate’ tab in upper right corner). Thank you all.
![]()
VRM: SB277 Road To Tyranny « Vaccine Resistance Movement on August 15, 2016
[…] VRM: Genetic Engineering & The Next Pandemic http://vaccineresistancemovement.org/?p=14588 […]
Joel Lord on February 16, 2016
There is a common misconception going around, that genetic engineering is somehow disconnected or separate from the whole Vaccine issue. Nothing could be further from the truth. The current wave of cases of Microcephaly you see unfolding in Brazil, is a direct result of the imposition of advanced vaccine technology interfering with the natural lifecycle of “wild” organisms in the environment. This is the evolution of decades of laboratory experimentation gone completely awry.
Genetic engineering represents the antithesis of holistic health, potentially the death of natural immunity itself, fueled by an Industry at height of its arrogance, so far-removed from the principles of natural immunity, the very concept of serving & protecting humanity is meaningless, compared to the greed and lustre of re-engineering the entire human species. VRM http://vaccineresistancemovement.org/?p=14588